Scientific Directorate of Epidemiology and Public Health, Sciensano, J. Wytsmanstraat 14, 1050 Brussels, Belgium.
Clinical Department of Laboratory Medicine and National Reference Center for Respiratory Pathogens, University Hospitals Leuven, 3000 Leuven, Belgium.
Viruses. 2022 Jun 14;14(6):1297. doi: 10.3390/v14061297.
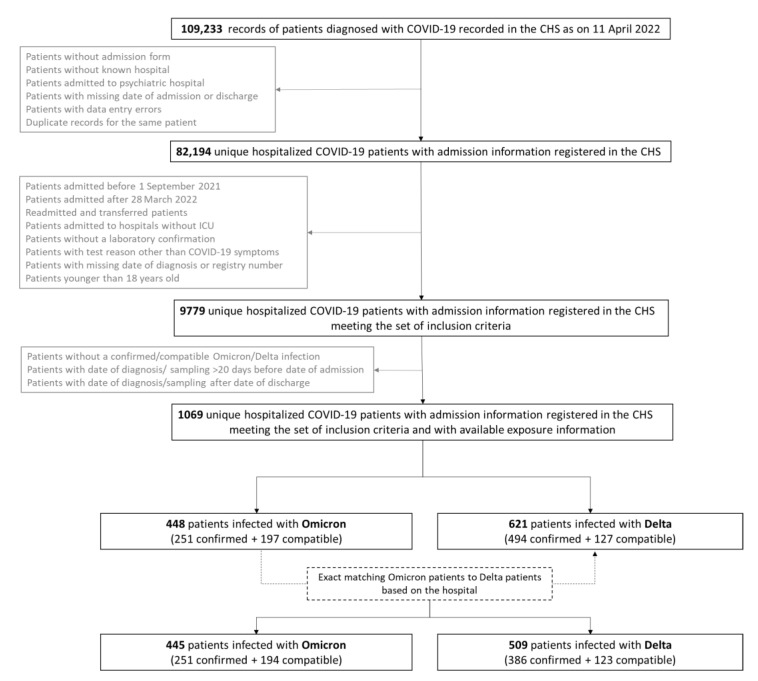
This retrospective multi-center matched cohort study assessed the risk for severe COVID-19 (combination of severity indicators), intensive care unit (ICU) admission, and in-hospital mortality in hospitalized patients when infected with the Omicron variant compared to when infected with the Delta variant. The study is based on a causal framework using individually-linked data from national COVID-19 registries. The study population consisted of 954 COVID-19 patients (of which, 445 were infected with Omicron) above 18 years old admitted to a Belgian hospital during the autumn and winter season 2021-2022, and with available viral genomic data. Patients were matched based on the hospital, whereas other possible confounders (demographics, comorbidities, vaccination status, socio-economic status, and ICU occupancy) were adjusted for by using a multivariable logistic regression analysis. The estimated standardized risk for severe COVID-19 and ICU admission in hospitalized patients was significantly lower (RR = 0.63; 95% CI (0.30; 0.97) and RR = 0.56; 95% CI (0.14; 0.99), respectively) when infected with the Omicron variant, whereas in-hospital mortality was not significantly different according to the SARS-CoV-2 variant (RR = 0.78, 95% CI (0.28-1.29)). This study demonstrates the added value of integrated genomic and clinical surveillance to recognize the multifactorial nature of COVID-19 pathogenesis.
本回顾性多中心匹配队列研究评估了与感染 Delta 变异株相比,感染奥密克戎变异株的住院患者发生严重 COVID-19(严重指标组合)、入住重症监护病房(ICU)和院内死亡的风险。该研究基于使用全国 COVID-19 登记处的个体关联数据的因果框架。研究人群包括 2021-2022 年秋冬季在比利时一家医院住院的 954 名 18 岁以上感染 COVID-19 的患者(其中 445 名感染奥密克戎),并具有可用的病毒基因组数据。患者根据医院进行匹配,而其他可能的混杂因素(人口统计学、合并症、疫苗接种状况、社会经济状况和 ICU 入住率)则通过多变量逻辑回归分析进行调整。感染奥密克戎变异株的住院患者发生严重 COVID-19 和入住 ICU 的估计标准化风险显著降低(RR = 0.63;95%CI(0.30;0.97)和 RR = 0.56;95%CI(0.14;0.99)),而根据 SARS-CoV-2 变异株,院内死亡率无显著差异(RR = 0.78,95%CI(0.28-1.29))。本研究表明,整合基因组和临床监测具有识别 COVID-19 发病机制的多因素性质的附加价值。