Liu Bao-Peng, Jia Cun-Xian, Qin Ping, Zhang Ying-Ying, Yu Yao-Kun, Luo Xiao, Li Shi-Xue
Department of Epidemiology, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, China.
Center for Suicide Prevention Research, Shandong University, Jinan, Shandong, China.
EClinicalMedicine. 2022 May 20;49:101461. doi: 10.1016/j.eclinm.2022.101461. eCollection 2022 Jul.
Longitudinal evidence for sociodemographic and clinic factors deviating risk for suicide and repetition following SH (self-harm) varied greatly.
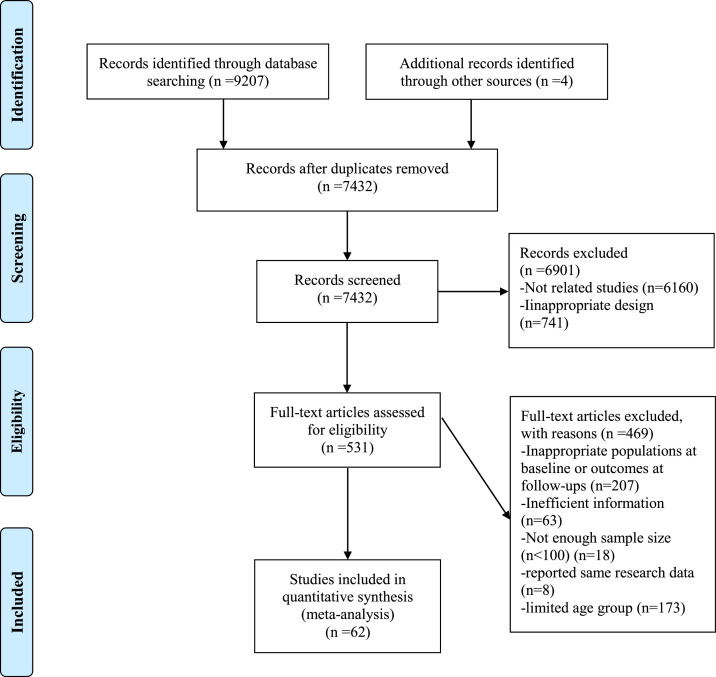
A comprehensive search of PubMed, Web of Science, EMBASE, and PsycINFO was conducted from January 1st, 2010 to April 5th, 2022. Longitudinal studies focusing on examining associating factors for suicide and repetition following SH were included. PROSPERO registration CRD42021248695.
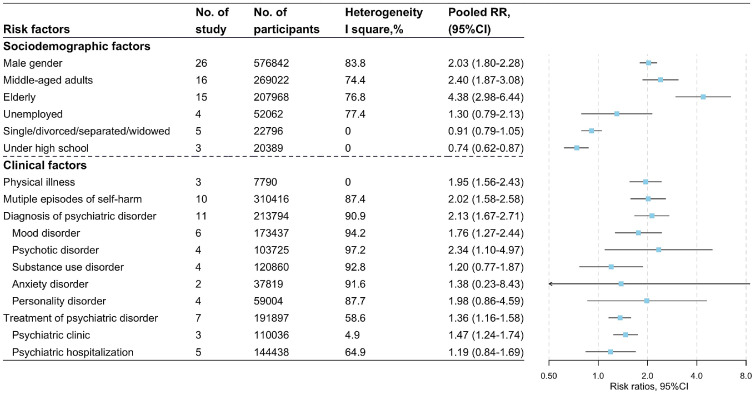
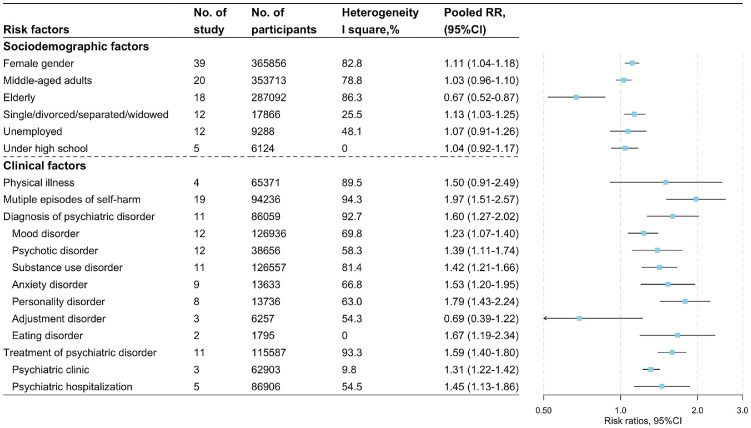
The present meta-analysis synthesized data from 62 studies published from Jan. 1st, 2010. The associating factors of SH repetition included female gender (RR, 95%CI: 1.11, 1.04-1.18, I=82.8%), the elderly (compared with adolescents and young adults, RR, 95%CI: 0.67, 0.52-0.87, I=86.3%), multiple episodes of SH (RR, 95%CI: 1.97, 1.51-2.57, I=94.3%), diagnosis (RR, 95%CI: 1.60, 1.27-2.02, I=92.7%) and treatment (RR, 95%CI: 1.59, 1.40-1.80, I=93.3%) of psychiatric disorder. Male gender (RR, 95%CI: 2.03, 1.80-2.28, I=83.8%), middle-aged adults (compared with adolescents and young adults, RR, 95%CI: 2.40, 1.87-3.08, I=74.4%), the elderly (compared with adolescents and young adults, RR, 95%CI: 4.38, 2.98-6.44, I=76.8%), physical illness (RR, 95%CI: 1.95, 1.56-2.43, I=0), multiple episodes of SH (RR, 95%CI: 2.02, 1.58-2.58, I=87.4%), diagnosis (RR, 95%CI: 2.13, 1.67-2.71, I=90.9%) and treatment (RR, 95%CI: 1.36, 1.16-1.58, I=58.6%) of psychiatric disorder were associated with increased risk of suicide following SH.
Due to the substantial heterogeneity for clinic factors of suicide and repetition following SH, these results need to be interpreted with caution. Clinics should pay more attention to the cases with SH repetition, especially with poor physical and psychiatric conditions.
This work was supported by National Natural Science Foundation of China (NSFC) [No: 82103954; 30972527; 81573233].
社会人口统计学和临床因素与自我伤害(SH)后自杀及重复自我伤害风险之间的纵向证据差异很大。
于2010年1月1日至2022年4月5日对PubMed、科学网、EMBASE和PsycINFO进行全面检索。纳入关注自我伤害后自杀及重复自我伤害相关因素的纵向研究。国际系统评价注册平台登记号CRD42021248695。
本荟萃分析综合了2010年1月1日以来发表的62项研究的数据。自我伤害重复的相关因素包括女性(风险比,95%置信区间:1.11,1.04 - 1.18,I² = 82.8%)、老年人(与青少年和年轻人相比,风险比,95%置信区间:0.67,0.52 - 0.87,I² = 86.3%)、多次自我伤害(风险比,95%置信区间:1.97,1.51 - 2.57,I² = 94.3%)、精神障碍诊断(风险比,95%置信区间:1.60,1.27 - 2.02,I² = 92.7%)和治疗(风险比,95%置信区间:1.59,1.40 - 1.80,I² = 93.3%)。男性(风险比,95%置信区间:2.03,1.80 - 2.28,I² = 83.8%)、中年成年人(与青少年和年轻人相比,风险比,95%置信区间:2.40,1.87 - 3.08,I² = 74.4%)、老年人(与青少年和年轻人相比,风险比,95%置信区间:4.38,2.98 - 6.44,I² = 76.8%)、躯体疾病(风险比,95%置信区间:1.95,1.56 - 2.43,I² = 0)、多次自我伤害(风险比,95%置信区间:2.02,1.58 - 2.58,I² = 87.4%)、精神障碍诊断(风险比,95%置信区间:2.13,1.67 - 2.71,I² = 90.9%)和治疗(风险比,95%置信区间:1.36,1.16 - 1.