Halpin David M G, Rabe Adrian Paul, Loke Wei Jie, Grieve Stacy, Daniele Patrick, Hwang Sanghee, Forsythe Anna
Respiratory Medicine, University of Exeter Medical School, College of Medicine and Health, University of Exeter, Exeter, Devon, UK.
Primary Care and Public Health, Imperial College London, London, UK.
J Asthma Allergy. 2022 Jun 17;15:811-825. doi: 10.2147/JAA.S360985. eCollection 2022.
There has been concern that asthma and chronic obstructive pulmonary disease [COPD] increase the risk of developing and exacerbating COVID-19. The effect of medications such as inhaled corticosteroids (ICS) and biologics on COVID-19 is unclear. This systematic literature review analyzed the published evidence on epidemiology and the burden of illness of asthma and COPD, and the use of baseline medicines among COVID-19 populations.
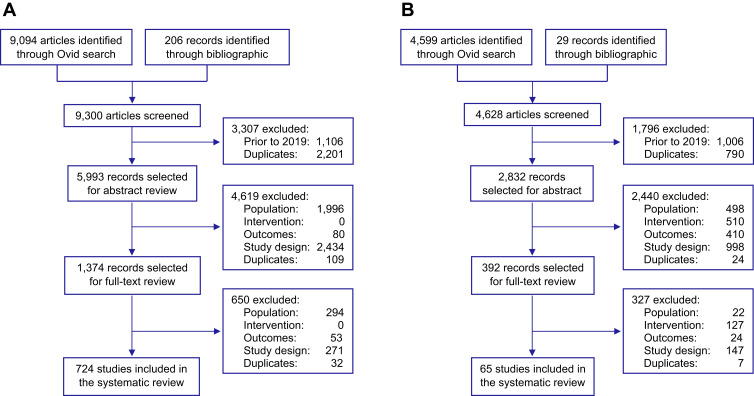
Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, Embase®, MEDLINE® and Cochrane were searched (January 2019-August 2021). The prevalence of asthma or COPD among COVID-19 populations was compared to the country-specific populations. Odds ratios (ORs) were estimated to compare healthcare resource utilization (HCRU) rates, and meta-analyses of outcomes were estimated from age-adjusted ORs (aORs) or hazard ratios (aHRs). Meta-analyses of COVID-19 outcomes were conducted using random effects models for binary outcomes.
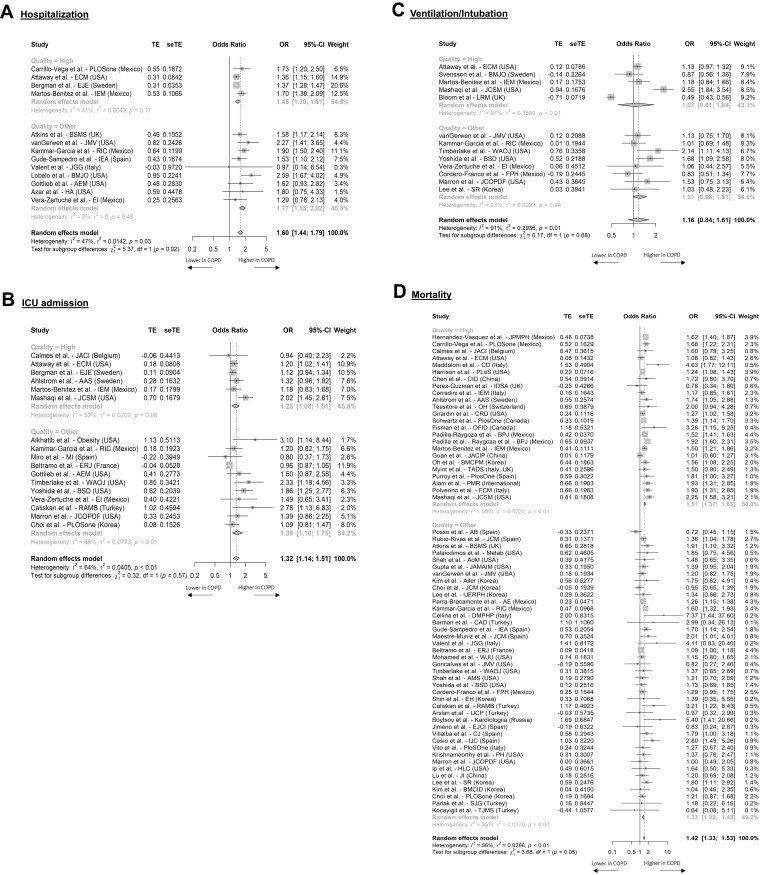
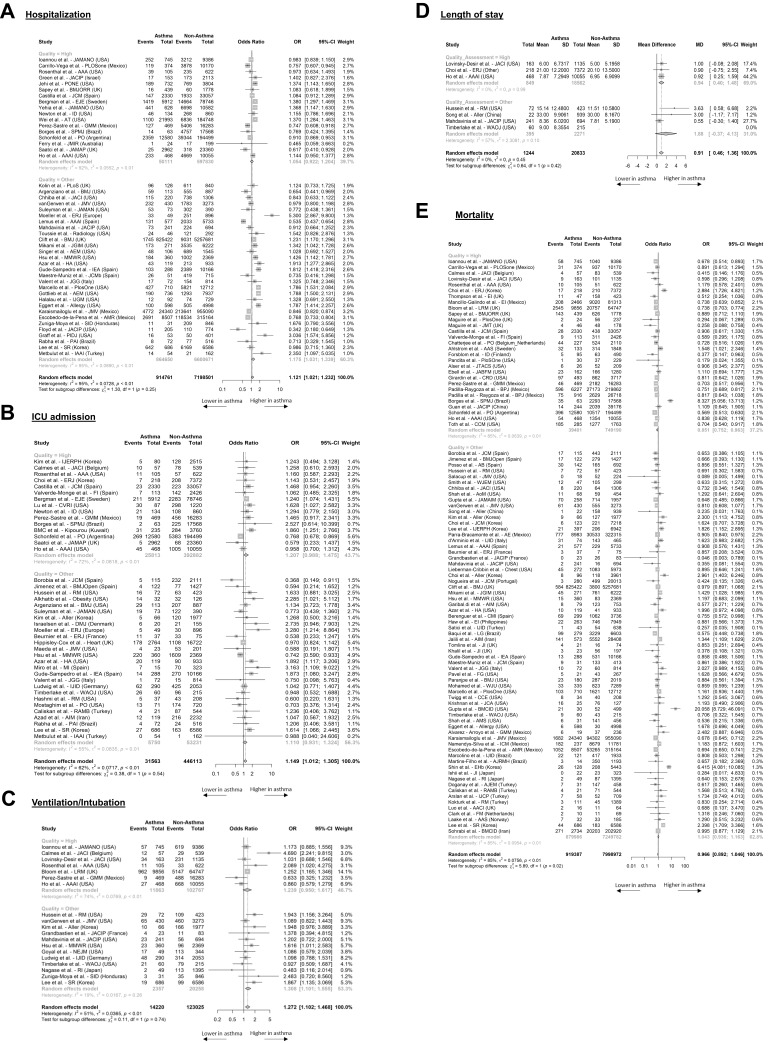
Given the number and heterogeneity of studies, only 183 high-quality studies were analyzed, which reported hospitalization, intensive care unit (ICU) admissions, ventilation/intubation, or mortality. Asthma patients were not at increased risk for COVID-19-related hospitalization (OR = 1.05, 95% CI: 0.92 to 1.20), ICU admission (OR = 1.21, 95% CI: 0.99 to 1.1.48), ventilation/intubation (OR = 1.24, 95% CI: 0.95 to 1.62), or mortality (OR = 0.85, 95% CI: 0.75 to 0.96). Accounting for confounding variables, COPD patients were at higher risk of hospitalization (aOR = 1.45, 95% CI: 1.30 to 1.61), ICU admission (aOR = 1.28, 95% CI: 1.08 to 1.51), and mortality (aOR = 1.41, 95% CI: 1.37 to 1.65). Sixty-five studies reported outcomes associated with ICS or biologic use. There was limited evidence that ICS or biologics significantly impacted the risk of SARS-CoV-2 infection, HCRU, or mortality in asthma or COPD patients.
In high-quality studies included, patients with asthma were not at significantly higher odds for adverse COVID-19-related outcomes, while patients with COPD were at higher odds. There was no clear evidence that baseline medication affected outcomes.
PROSPERO (CRD42021233963).
一直有人担心哮喘和慢性阻塞性肺疾病(COPD)会增加感染和加重2019冠状病毒病(COVID-19)的风险。吸入性糖皮质激素(ICS)和生物制剂等药物对COVID-19的影响尚不清楚。本系统文献综述分析了已发表的关于哮喘和COPD的流行病学和疾病负担,以及COVID-19人群中基线药物使用情况的证据。
按照系统评价和Meta分析的首选报告项目指南,检索了Embase®、MEDLINE®和Cochrane数据库(2019年1月至2021年8月)。将COVID-19人群中哮喘或COPD的患病率与特定国家人群进行比较。估计比值比(OR)以比较医疗资源利用(HCRU)率,并根据年龄调整后的OR(aOR)或风险比(aHR)对结局进行Meta分析。使用二元结局的随机效应模型对COVID-19结局进行Meta分析。
鉴于研究数量和异质性,仅分析了183项高质量研究,这些研究报告了住院、重症监护病房(ICU)入院、通气/插管或死亡率。哮喘患者与COVID-19相关的住院风险未增加(OR = 1.05,95% CI:0.92至1.20)、ICU入院风险(OR = 1.21,95% CI:0.99至1.48)、通气/插管风险(OR = 1.24,95% CI:0.95至1.62)或死亡风险(OR = 0.85,95% CI:0.75至0.96)。考虑到混杂变量,COPD患者的住院风险更高(aOR = 1.45,95% CI:1.30至1.61)、ICU入院风险(aOR = 1.28,95% CI:1.08至1.51)和死亡风险(aOR = 1.41,95% CI:1.37至1.65)。65项研究报告了与使用ICS或生物制剂相关的结局。仅有有限的证据表明ICS或生物制剂会显著影响哮喘或COPD患者感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的风险、HCRU或死亡率。
在纳入的高质量研究中,哮喘患者出现与COVID-19相关不良结局的几率并未显著更高,而COPD患者的几率更高。没有明确证据表明基线用药会影响结局。
PROSPERO(CRD42021233963)