Division of General Pediatric Surgery, Johns Hopkins Children's Center, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Pediatric Radiology, Children's Mercy Hospital, University of Missouri-Kansas City School of Medicine, Kansas City.
JAMA Netw Open. 2022 Jun 1;5(6):e2219814. doi: 10.1001/jamanetworkopen.2022.19814.
The ability of computed tomography (CT) to distinguish between benign congenital lung malformations and malignant cystic pleuropulmonary blastomas (PPBs) is unclear.
To assess whether chest CT can detect malignant tumors among postnatally detected lung lesions in children.
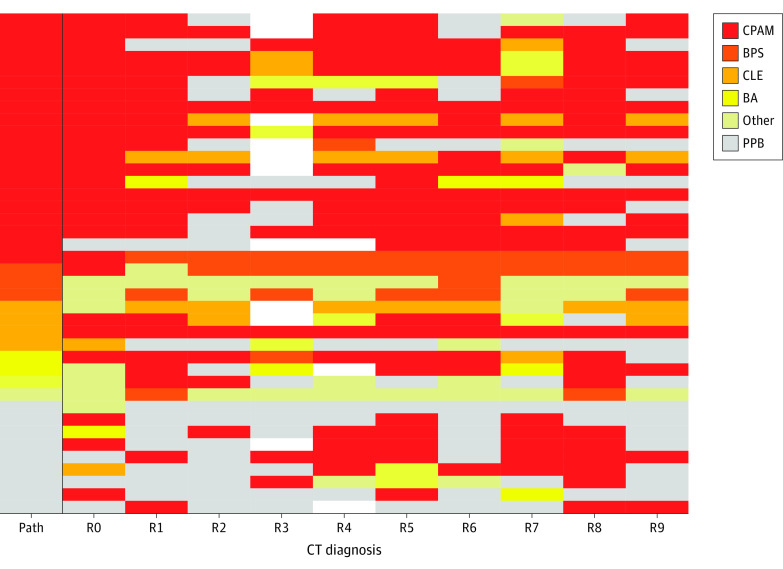
DESIGN, SETTING, AND PARTICIPANTS: This retrospective multicenter case-control study used a consortium database of 521 pathologically confirmed primary lung lesions from January 1, 2009, through December 31, 2015, to assess diagnostic accuracy. Preoperative CT scans of children with cystic PPB (cases) were selected and age-matched with CT scans from patients with postnatally detected congenital lung malformations (controls). Statistical analysis was performed from January 18 to September 6, 2020. Preoperative CT scans were interpreted independently by 9 experienced pediatric radiologists in a blinded fashion and analyzed from January 24, 2019, to September 6, 2020.
Accuracy, sensitivity, and specificity of CT in correctly identifying children with malignant tumors.
Among 477 CT scans identified (282 boys [59%]; median age at CT, 3.6 months [IQR, 1.2-7.2 months]; median age at resection, 6.9 months [IQR, 4.2-12.8 months]), 40 cases were extensively reviewed; 9 cases (23%) had pathologically confirmed cystic PPB. The median age at CT was 7.3 months (IQR, 2.9-22.4 months), and median age at resection was 8.7 months (IQR, 5.0-24.4 months). The sensitivity of CT for detecting PPB was 58%, and the specificity was 83%. High suspicion for malignancy correlated with PPB pathology (odds ratio, 13.5; 95% CI, 2.7-67.3; P = .002). There was poor interrater reliability (κ = 0.36 [range, 0.06-0.64]; P < .001) and no significant difference in specific imaging characteristics between PPB and benign cystic lesions. The overall accuracy rate for distinguishing benign vs malignant lesions was 81%.
This study suggests that chest CT, the current criterion standard imaging modality to assess the lung parenchyma, may not accurately and reliably distinguish PPB from benign congenital lung malformations in children. In any cystic lung lesion without a prenatal diagnosis, operative management to confirm pathologic diagnosis is warranted.
计算机断层扫描(CT)区分良性先天性肺畸形和恶性囊性胸膜肺母细胞瘤(PPB)的能力尚不清楚。
评估 CT 是否可用于检测儿童出生后肺部病变中的恶性肿瘤。
设计、地点和参与者:本回顾性多中心病例对照研究使用了 2009 年 1 月 1 日至 2015 年 12 月 31 日的一个联盟数据库,该数据库包含 521 例经病理证实的原发性肺病变,以评估诊断准确性。选择囊性 PPB(病例)患儿的术前 CT 扫描,并与出生后发现的先天性肺畸形(对照)患儿的 CT 扫描进行年龄匹配。统计分析于 2020 年 1 月 18 日至 9 月 6 日进行。9 名经验丰富的儿科放射科医生独立对术前 CT 扫描进行了盲法解读,并于 2019 年 1 月 24 日至 9 月 6 日进行了分析。
CT 正确识别恶性肿瘤患儿的准确性、敏感性和特异性。
共确定了 477 份 CT 扫描(282 名男孩[59%];CT 时的中位年龄为 3.6 个月[IQR,1.2-7.2 个月];切除术时的中位年龄为 6.9 个月[IQR,4.2-12.8 个月]),对 40 份 CT 扫描进行了广泛复查;9 例(23%)经病理证实为囊性 PPB。CT 时的中位年龄为 7.3 个月(IQR,2.9-22.4 个月),切除术时的中位年龄为 8.7 个月(IQR,5.0-24.4 个月)。CT 对 PPB 的检出敏感性为 58%,特异性为 83%。高度怀疑恶性肿瘤与 PPB 病理学相关(比值比,13.5;95%CI,2.7-67.3;P = .002)。存在较差的观察者间可靠性(κ = 0.36[范围,0.06-0.64];P < .001),且 PPB 和良性囊性病变之间的特异性影像学特征无显著差异。区分良性与恶性病变的总准确率为 81%。
本研究表明,胸部 CT 是目前评估肺实质的标准影像学方法,但可能无法准确可靠地区分儿童的 PPB 和良性先天性肺畸形。在任何没有产前诊断的囊性肺病变中,都需要手术管理以确认病理诊断。