Academic Rheumatology, University of Nottingham, Nottingham, UK.
Department of Infectious Disease, Imperial College London, London, UK; Lung Division, Royal Brompton and Harefield Hospitals, Guy's and St Thomas' National Health Service (NHS) Foundation Trust, London, UK.
Lancet Respir Med. 2022 Sep;10(9):840-850. doi: 10.1016/S2213-2600(22)00186-2. Epub 2022 Jun 27.
Immunosuppressive treatments inhibit vaccine-induced immunity against SARS-CoV-2. We evaluated whether a 2-week interruption of methotrexate treatment immediately after the COVID-19 vaccine booster improved antibody responses against the S1 receptor-binding domain (S1-RBD) of the SARS-CoV-2 spike protein compared with uninterrupted treatment in patients with immune-mediated inflammatory diseases.
We did an open-label, prospective, two-arm, parallel-group, multicentre, randomised, controlled, superiority trial in 26 hospitals in the UK. We recruited adults from rheumatology and dermatology clinics who had been diagnosed with an immune-mediated inflammatory disease (eg, rheumatoid arthritis, psoriasis with or without arthritis, axial spondyloarthritis, atopic dermatitis, polymyalgia rheumatica, and systemic lupus erythematosus) and who were taking low-dose weekly methotrexate (≤25 mg per week) for at least 3 months. Participants also had to have received two primary vaccine doses from the UK COVID-19 vaccination programme. We randomly assigned the participants (1:1), using a centralised validated computer randomisation program, to suspend methotrexate treatment for 2 weeks immediately after their COVID-19 booster (suspend methotrexate group) or to continue treatment as usual (continue methotrexate group). Participants, investigators, clinical research staff, and data analysts were unmasked, while researchers doing the laboratory analyses were masked to group assignment. The primary outcome was S1-RBD antibody titres 4 weeks after receiving the COVID-19 booster vaccine dose, assessed in the intention-to-treat population. This trial is registered with ISRCT, ISRCTN11442263; following the pre-planned interim analysis, recruitment was stopped early.
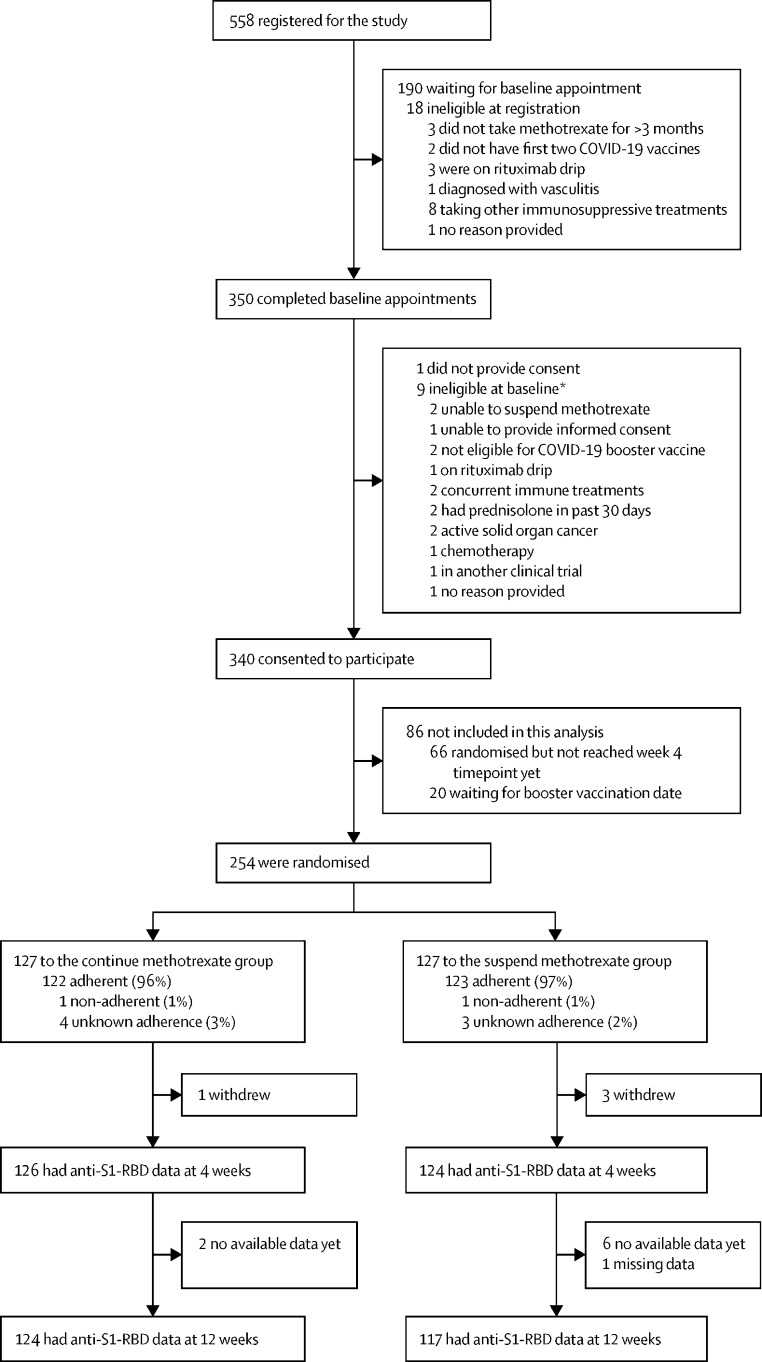
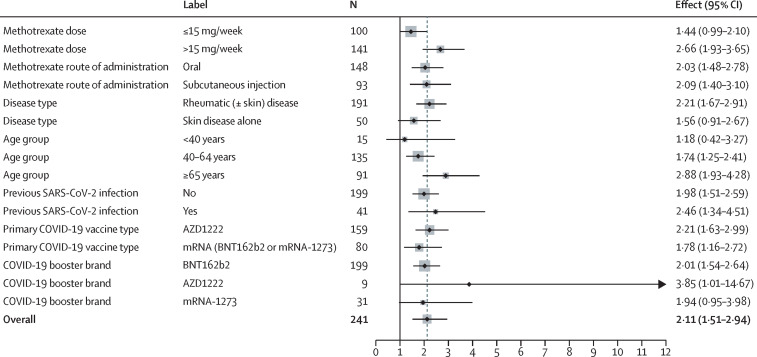
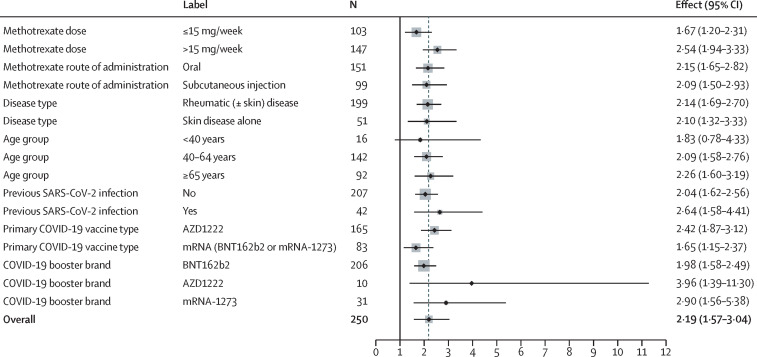
Between Sept 30, 2021 and March 3, 2022, we recruited 340 participants, of whom 254 were included in the interim analysis and had been randomly assigned to one of the two groups: 127 in the continue methotrexate group and 127 in the suspend methotrexate group. Their mean age was 59·1 years, 155 (61%) were female, 130 (51%) had rheumatoid arthritis, and 86 (34%) had psoriasis with or without arthritis. After 4 weeks, the geometric mean S1-RBD antibody titre was 22 750 U/mL (95% CI 19 314-26 796) in the suspend methotrexate group and 10 798 U/mL (8970-12 997) in the continue methotrexate group, with a geometric mean ratio (GMR) of 2·19 (95% CI 1·57-3·04; p<0·0001; mixed-effects model). The increased antibody response in the suspend methotrexate group was consistent across methotrexate dose, administration route, type of immune-mediated inflammatory disease, age, primary vaccination platform, and history of SARS-CoV-2 infection. There were no intervention-related serious adverse events.
A 2-week interruption of methotrexate treatment for people with immune-mediated inflammatory diseases resulted in enhanced boosting of antibody responses after COVID-19 vaccination. This intervention is simple, low-cost, and easy to implement, and could potentially translate to increased vaccine efficacy and duration of protection for susceptible groups.
National Institute for Health and Care Research.
免疫抑制治疗抑制了 SARS-CoV-2 疫苗诱导的免疫。我们评估了在 COVID-19 疫苗加强针后立即中断甲氨蝶呤治疗(中断治疗组)与继续治疗(继续治疗组)相比,是否会改善接受免疫介导的炎症性疾病治疗的患者对 SARS-CoV-2 刺突蛋白 S1 受体结合域(S1-RBD)的抗体反应。
我们在英国 26 家医院进行了一项开放性、前瞻性、双盲、平行组、多中心、随机、对照、优效性试验。我们招募了在风湿病和皮肤科诊所被诊断为免疫介导的炎症性疾病(例如类风湿关节炎、有或没有关节炎的银屑病、轴向脊柱关节炎、特应性皮炎、多发性肌痛和系统性红斑狼疮)并接受低剂量每周甲氨蝶呤(每周 25 毫克或以下)治疗至少 3 个月的成年人。参与者还必须接受过英国 COVID-19 疫苗接种计划的两次主要疫苗接种。我们使用中央验证的计算机随机化程序将参与者(1:1)随机分配,在 COVID-19 加强针后立即中断(中断甲氨蝶呤组)或继续治疗(继续甲氨蝶呤组)。参与者、研究者、临床研究人员和数据分析人员被揭盲,而进行实验室分析的研究人员则对分组情况进行盲法。主要结局是在接受 COVID-19 加强针后 4 周时的 S1-RBD 抗体滴度,在意向治疗人群中进行评估。该试验在 ISRCTN 注册,ISRCTN11442263;在计划的中期分析后,提前停止了招募。
2021 年 9 月 30 日至 2022 年 3 月 3 日,我们招募了 340 名参与者,其中 254 名被纳入中期分析,并被随机分配到两组之一:继续甲氨蝶呤组 127 名,中断甲氨蝶呤组 127 名。他们的平均年龄为 59.1 岁,155 名(61%)为女性,130 名(51%)患有类风湿关节炎,86 名(34%)患有有或没有关节炎的银屑病。4 周后,中断甲氨蝶呤组的 S1-RBD 抗体滴度几何平均值为 22750 U/mL(95%CI 19314-26796),继续甲氨蝶呤组为 10798 U/mL(8970-12997),几何平均比(GMR)为 2.19(95%CI 1.57-3.04;p<0.0001;混合效应模型)。中断甲氨蝶呤组的抗体反应增强在甲氨蝶呤剂量、给药途径、免疫介导的炎症性疾病类型、年龄、主要疫苗接种平台和 SARS-CoV-2 感染史方面均一致。没有与干预相关的严重不良事件。
中断免疫介导的炎症性疾病患者的甲氨蝶呤治疗 2 周会增强 COVID-19 疫苗接种后的抗体增强反应。这种干预措施简单、低成本且易于实施,可能会增加易感人群的疫苗效力和保护持续时间。
英国国家卫生与保健研究院。