National Heart and Lung Institute, Imperial College London, London, UK
NIHR Imperial Biomedical Research Centre, London, UK.
BMJ Open. 2022 Jun 30;12(6):e059122. doi: 10.1136/bmjopen-2021-059122.
To evaluate the association between having concomitant chronic obstructive pulmonary disease (COPD) or asthma, and in-patient mortality and post-discharge management among patients hospitalised for acute heart failure (HF).
Data were obtained from patients enrolled in the National Heart Failure Audit.
217 329 patients hospitalised for HF in England-Wales between March 2012 and 2018.
In-hospital mortality, referrals to cardiology follow-up and prescriptions for HF medications were compared between patients with comorbid COPD (COPD-HF) or asthma (asthma-HF) versus HF-alone using mixed-effects logistic regression.
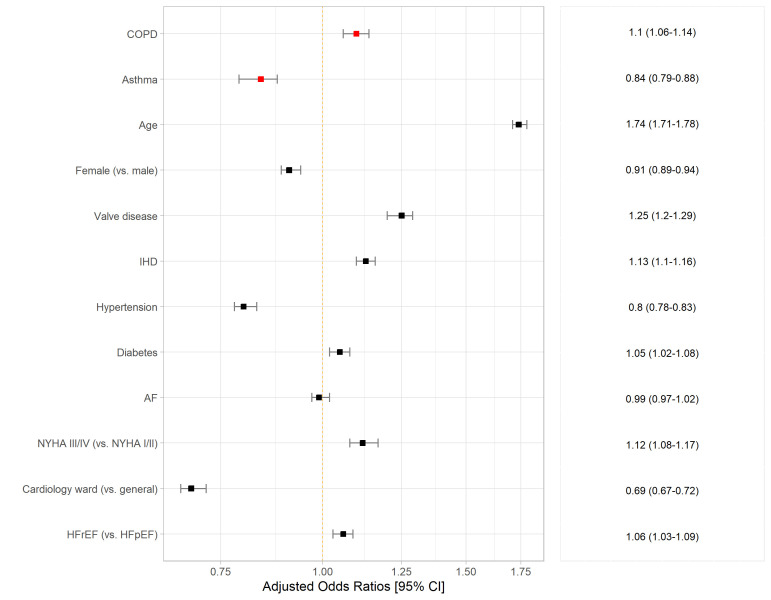
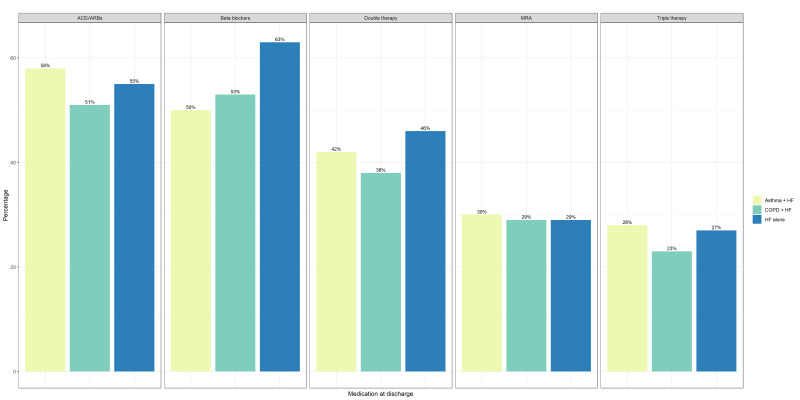
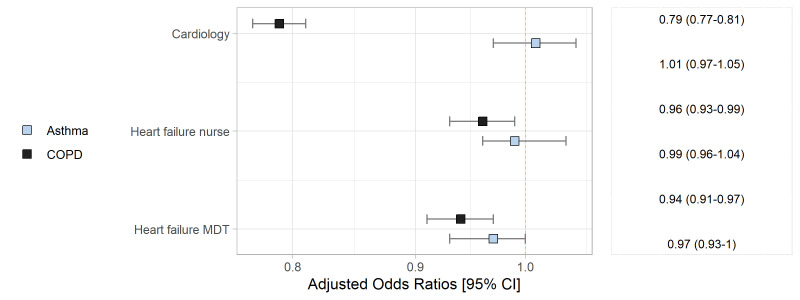
Patients with COPD-HF were more likely to die during hospitalisation, and those with asthma-HF had a reduced likelihood of death, compared with patients who had HF-alone ((adjusted)OR, 95% CI: 1.10, 1.06 to 1.14 and OR, 95% CI: 0.84, 0.79 to 0.88). In patients who survived to discharge, referral to HF follow-up services differed between groups: patients with COPD-HF had reduced odds of cardiology follow-up (OR, 95% CI 0.79, 0.77 to 0.81), while cardiology referral odds for asthma-HF were similar to HF-alone. Overall, proportions of HF medication prescriptions at discharge were low for both COPD-HF and asthma-HF groups, particularly prescriptions for beta-blockers.
In this nationwide analysis, we showed that COPD and asthma significantly impact the clinical course in patients hospitalised for HF. COPD is associated with higher in-patient mortality and lower cardiology referral odds, while COPD and asthma are both associated with lower use of prognostic HF therapies on discharge. These data highlight therapeutic gaps and a need for better integration of cardiopulmonary services to improve healthcare provision for patients with HF and coexisting respiratory disease.
评估同时患有慢性阻塞性肺疾病(COPD)或哮喘与急性心力衰竭(HF)住院患者的住院死亡率和出院后管理之间的关联。
数据来自英格兰和威尔士 2012 年 3 月至 2018 年期间纳入国家心力衰竭审计的患者。
217329 名因 HF 住院的患者。
使用混合效应逻辑回归比较了合并 COPD(COPD-HF)或哮喘(哮喘-HF)与单纯 HF 的患者之间的住院死亡率、转至心脏病学随访以及 HF 药物处方。
与单纯 HF 的患者相比,COPD-HF 患者在住院期间更有可能死亡,而哮喘-HF 患者死亡的可能性降低(调整后 OR,95%CI:1.10,1.06 至 1.14 和 OR,95%CI:0.84,0.79 至 0.88)。在存活至出院的患者中,各组之间转至 HF 随访服务的情况有所不同:COPD-HF 患者心脏病学随访的可能性降低(OR,95%CI 0.79,0.77 至 0.81),而哮喘-HF 的心脏病学转介可能性与单纯 HF 相似。总体而言,COPD-HF 和哮喘-HF 组出院时 HF 药物处方的比例均较低,特别是β受体阻滞剂的处方。
在这项全国性分析中,我们表明 COPD 和哮喘显著影响 HF 住院患者的临床病程。COPD 与更高的住院死亡率和更低的心脏病学转诊可能性相关,而 COPD 和哮喘均与出院时使用预测 HF 治疗的可能性降低相关。这些数据突出了治疗空白,并需要更好地整合心肺服务,以改善 HF 和并存呼吸系统疾病患者的医疗服务。