College of Education for the Future, Beijing Normal University, China.
The National Clinical Research Center for Mental Disorders & Beijing Key Laboratory of Mental Disorders Beijing Anding Hospital & the Advanced Innovation Center for Human Brain Protection, Capital Medical University, School of Mental Health, Beijing, China.
J Affect Disord. 2022 Oct 1;314:193-200. doi: 10.1016/j.jad.2022.06.051. Epub 2022 Jun 30.
Mental health problems are common among clinicians working in public hospitals even in the late stage of the COVID-19 pandemic. Network analysis is a novel approach to explore interactions between mental health problems at the symptom level. This study examined the network structure of comorbid depression and anxiety and their associations with quality of life (QOL) among hospital clinicians in China during the late stage of the COVID-19 pandemic.
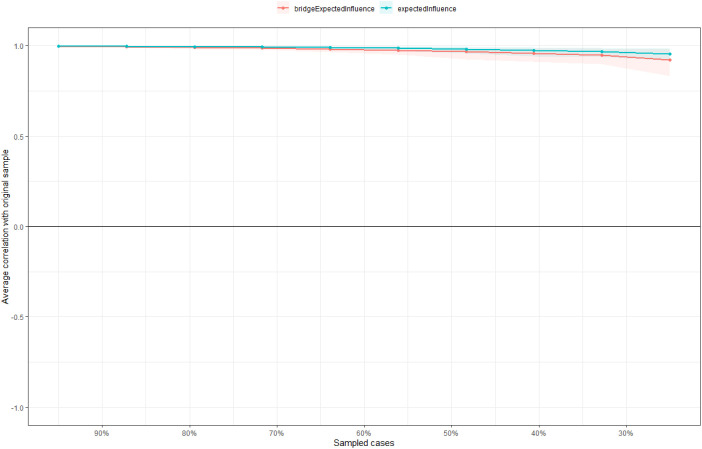
A total of 4931 participants were recruited from October 13 to 22, 2020. The nine-item Patient Health Questionnaire (PHQ-9), seven-item Generalized Anxiety Disorder Scale (GAD-7), and the World Health Organization Quality of Life Questionnaire-Brief Version (WHOQOL-BREF) were used to measure depressive and anxiety symptoms, and QOL, respectively. Central and bridge symptoms were identified with centrality and bridge centrality indices, respectively. Network stability was examined using the case-dropping procedure.
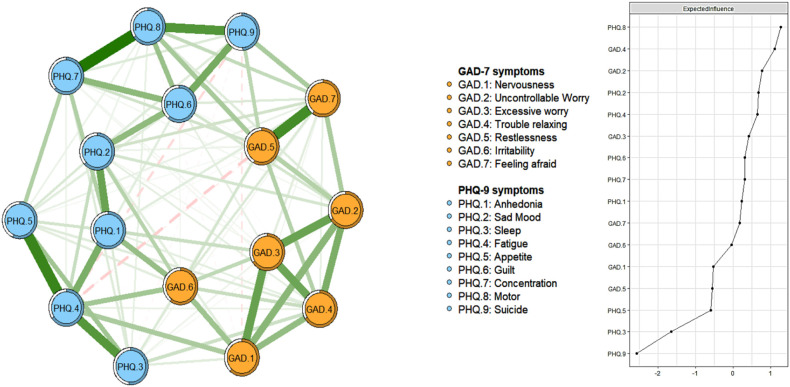
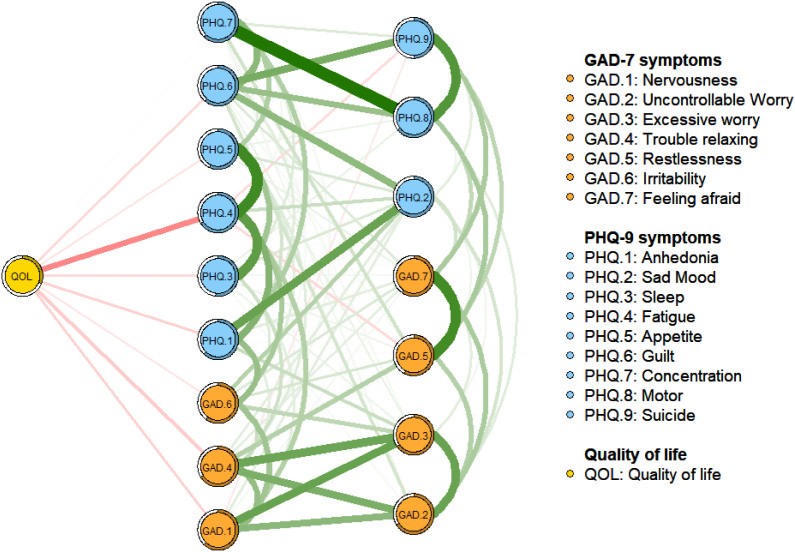
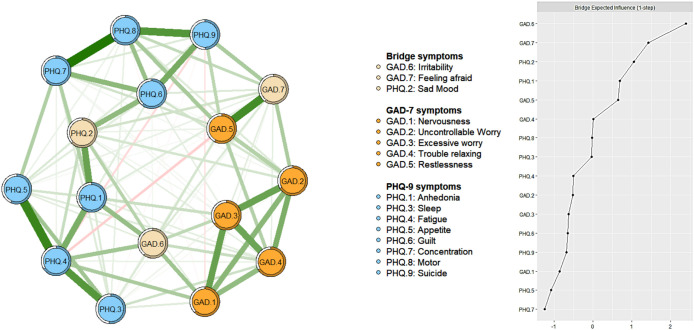
The prevalence of depression (defined as PHQ-9 total score ≥ 5) was 35.1 % [95 % confidence interval (CI) = 33.73-36.41 %)], the prevalence of anxiety (GAD-7 total score ≥ 5) was 32.5 % (95 % CI = 31.20-33.84 %), while the prevalence of comorbid depression and anxiety was 26.9 % (95 % CI = 25.7-28.2 %). "Impaired motor skills", "Trouble relaxing" and "Uncontrollable worry" were the central symptoms in the whole depression-anxiety network. "Irritability", "Feeling afraid" and "Sad mood" were the most key bridge symptoms linking depression and anxiety. Three symptoms ("Fatigue", "Trouble relaxing" and "Nervousness") were the most strongly and negatively associated with QOL. Neither gender nor the experiences of caring for COVID-19 patients was associated with network global strength, distribution of edge weights or individual edge weights.
The causality between variables could not be established. Depressive and anxiety symptoms were assessed by self-report measures, which may result in recall bias and limitations in capturing clinical phenomena.
Both the central (i.e., "Impaired motor skills", "Trouble relaxing" and "Uncontrollable worry") and bridge symptoms (i.e., "Irritability", "Feeling afraid" and "Sad mood") identified in this network analysis should be targeted in specific treatment and preventive measures for comorbid depressive and anxiety symptoms among clinicians in the late stage of the pandemic. Furthermore, "Fatigue", "Trouble relaxing" and "Nervousness" are key symptoms to address to improve clinicians' QOL.
即使在 COVID-19 大流行后期,在公立医院工作的临床医生中也普遍存在心理健康问题。网络分析是一种探索症状水平上心理健康问题相互作用的新方法。本研究调查了中国 COVID-19 大流行后期医院临床医生中并发抑郁和焦虑的共病网络结构及其与生活质量(QOL)的关系。
共有 4931 名参与者于 2020 年 10 月 13 日至 22 日招募。使用 9 项患者健康问卷(PHQ-9)、7 项广泛性焦虑症量表(GAD-7)和世界卫生组织生活质量量表-简明版(WHOQOL-BREF)分别测量抑郁和焦虑症状以及生活质量。使用中心度和桥中心度指数分别确定中心和桥症状。使用病例删除程序检查网络稳定性。
抑郁的患病率(定义为 PHQ-9 总分≥5)为 35.1%[95%置信区间(CI)=33.73-36.41%],焦虑的患病率(GAD-7 总分≥5)为 32.5%(95%CI=31.20-33.84%),而并发抑郁和焦虑的患病率为 26.9%(95%CI=25.7-28.2%)。“运动技能受损”、“放松困难”和“无法控制的担忧”是整个抑郁-焦虑网络中的中心症状。“易怒”、“感到害怕”和“悲伤情绪”是连接抑郁和焦虑的最关键的桥接症状。三个症状(“疲劳”、“放松困难”和“紧张”)与 QOL 呈最强和负相关。性别和照顾 COVID-19 患者的经历与网络全局强度、边缘权重分布或个体边缘权重均无关联。
变量之间的因果关系无法建立。抑郁和焦虑症状是通过自我报告措施评估的,这可能导致回忆偏倚和限制对临床现象的捕捉。
本网络分析中确定的中心(即“运动技能受损”、“放松困难”和“无法控制的担忧”)和桥接症状(即“易怒”、“感到害怕”和“悲伤情绪”)都应该作为针对大流行后期临床医生并发抑郁和焦虑症状的特定治疗和预防措施的目标。此外,“疲劳”、“放松困难”和“紧张”是改善临床医生生活质量的关键症状。