Tilden Ellen L, Snowden Jonathan M, Bovbjerg Marit L, Cheyney Melissa, Lapidus Jodi, Wiedrick Jack, Caughey Aaron B
Department Nurse-Midwifery, School of Nursing, Oregon Health and Science University , 577, 3181 SW Sam Jackson Park Rd., Portland, OR 97214, USA.
UpLift Lab, Oregon State University, Corvallis, OR, USA.
EClinicalMedicine. 2022 May 22;48:101447. doi: 10.1016/j.eclinm.2022.101447. eCollection 2022 Jun.
Friedman's curve, despite acknowledged limitations, has greatly influenced labour management. Interventions to hasten birth are now ubiquitous, challenging the contemporary study of normal labour. Our primary purpose was to characterise normal active labour and pushing durations in a large, contemporary sample experiencing minimal intervention, stratified by parity, age, and body mass index (BMI).
This is a secondary analysis of the national, validated Midwives Alliance of North America 4·0 (MANA Stats) data registry ( = 75,243), prospectively collected between Jan 1, 2012 and Dec 31, 2018 to describe labour and birth in home and birth center settings where common obstetric interventions [i.e., oxytocin, planned cesarean] are not available. The MANA Stats cohort includes pregnant people who intended birth in these settings and prospectively collects labour and birth processes and outcomes regardless of where birth or postpartum care ultimately occurs. Survival curves were calculated to estimate labour duration percentiles (e.g. 10th, 50th, 90th, and others of interest), by parity and sub-stratified by age and BMI.
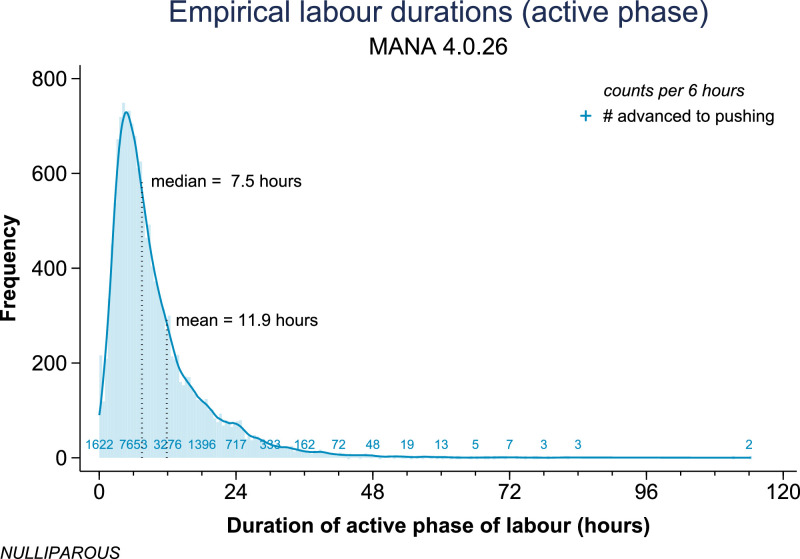
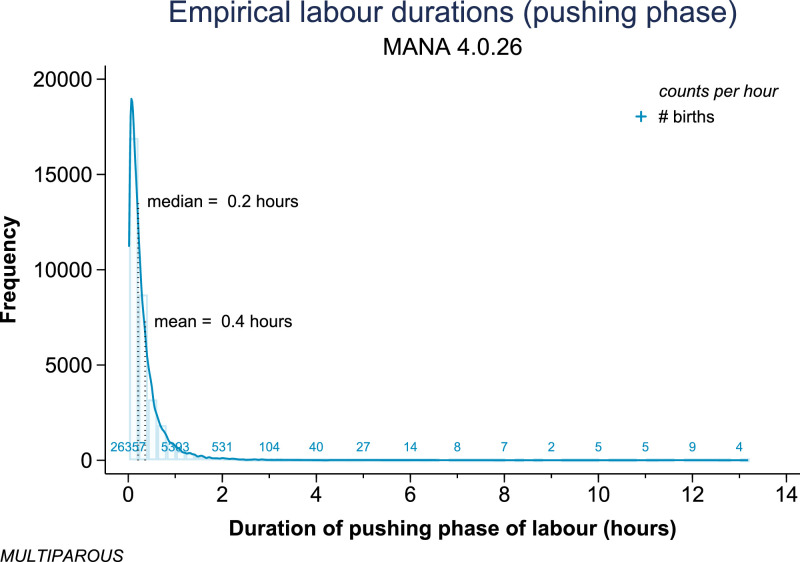
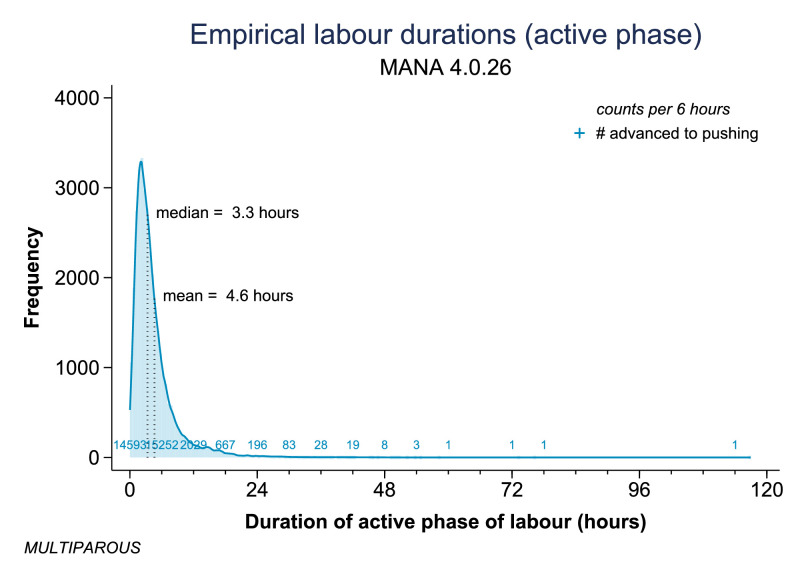
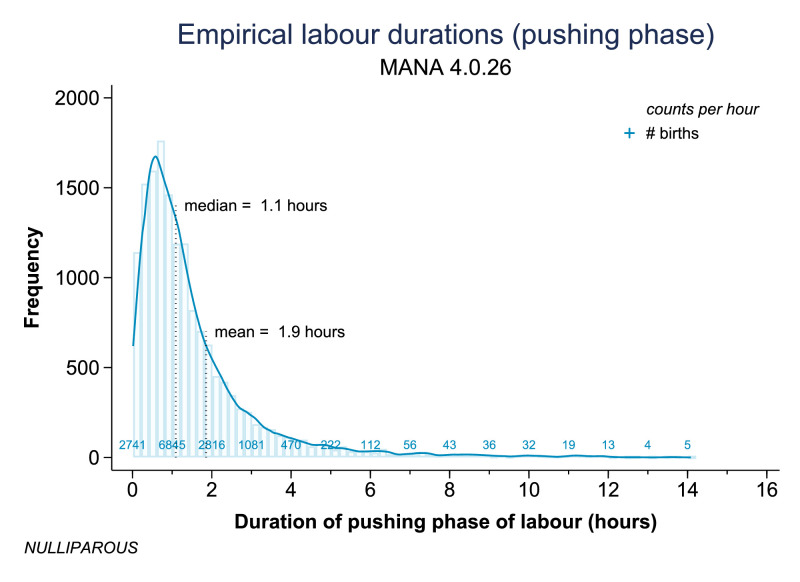
Compared to multiparous women ( = 32,882), nulliparous women ( = 15,331) had significantly longer active labour [e.g., median 7.5 vs. 3.3 h; 95th percentile 34.8 vs. 12.0 h] and significantly longer pushing phase [e.g., median 1.1 vs. 0.2 h; 95th percentile 5.5 vs. 1.1 h]. Among nulliparous women, maternal age >35 was associated with longer active first stage of labour and longer pushing phase, and BMI >30 kg/m² was associated with a longer active first stage of labour but a shorter pushing phase. Patterns among multiparous women were different, with those >35 years of age experiencing a slightly more rapid active labour and no difference in pushing duration, and those with BMI >30 kg/m² experiencing a slightly longer active labour but, similarly, no difference in pushing duration.
Nulliparous women had significantly longer active first stage and pushing phase durations than multiparous women, with further variation noted by age and by BMI. Contemporary US women with low-risk pregnancies who intended birth in settings absent common obstetric interventions and in spontaneous labour with a live, vertex, term, singleton, non-anomalous fetus experienced labour durations that were often longer than prior characterizations, particularly among nulliparous women. Results overcome prior and current sampling limitations to refine understanding of normal labour durations and time thresholds signaling 'labour dystocia'.
OHSU Nursing Innovation and OHSU University Shared Resources.
弗里德曼曲线尽管存在公认的局限性,但对产程管理产生了重大影响。如今,加速分娩的干预措施无处不在,这对正常产程的当代研究提出了挑战。我们的主要目的是在一个经历最少干预的大型当代样本中,按产次、年龄和体重指数(BMI)分层,描述正常活跃期产程和第二产程的时长。
这是对经过验证的北美助产士联盟4.0(MANA Stats)全国数据登记处(n = 75,243)的二次分析,该数据于2012年1月1日至2018年12月31日期间前瞻性收集,用于描述家庭和分娩中心环境下的产程和分娩情况,这些环境中没有常见的产科干预措施(即缩宫素、计划剖宫产)。MANA Stats队列包括打算在这些环境中分娩的孕妇,并前瞻性收集产程和分娩过程及结果,无论最终分娩或产后护理发生在哪里。计算生存曲线以估计产程时长百分位数(如第10、50、90百分位数及其他感兴趣的百分位数),按产次分层,并按年龄和BMI进一步分层。
与经产妇(n = 32,882)相比,初产妇(n = 15,331)的活跃期产程明显更长[例如,中位数7.5小时对3.3小时;第95百分位数34.8小时对12.0小时],第二产程也明显更长[例如,中位数1.1小时对0.2小时;第95百分位数5.5小时对1.1小时]。在初产妇中,母亲年龄>35岁与活跃期第一产程更长和第二产程更长有关,BMI>30kg/m²与活跃期第一产程更长但第二产程更短有关。经产妇的模式不同,年龄>35岁的经产妇活跃期产程稍快,第二产程时长无差异,BMI>30kg/m²的经产妇活跃期产程稍长,但同样第二产程时长无差异。
初产妇的活跃期第一产程和第二产程时长明显长于经产妇,年龄和BMI进一步导致差异。在美国,有低风险妊娠且打算在没有常见产科干预措施的环境中自然分娩、活产、头位、足月、单胎、无畸形胎儿的当代女性,其产程时长通常比之前描述的更长,尤其是初产妇。研究结果克服了之前和当前的抽样局限性,有助于更准确地理解正常产程时长以及提示“产程难产”的时间阈值。
俄勒冈健康与科学大学护理创新项目及俄勒冈健康与科学大学大学共享资源。