Health Economics and Outcomes Research, Boehringer Ingelheim Pharmaceuticals, Inc, Ridgefield, CT, USA.
Department of Biostatistics and Data Science, Division of Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, NC, USA.
Int J Chron Obstruct Pulmon Dis. 2022 Jun 29;17:1483-1494. doi: 10.2147/COPD.S355772. eCollection 2022.
Patients with chronic obstructive pulmonary disease (COPD) can have low peak inspiratory flow (PIF), especially after hospitalization for acute exacerbation of COPD (AECOPD).
To characterize patients hospitalized for AECOPD, and to assess the prevalence of low PIF, changes in PIF after hospitalization, and the association of low PIF with healthcare resource utilization (HRU) outcomes.
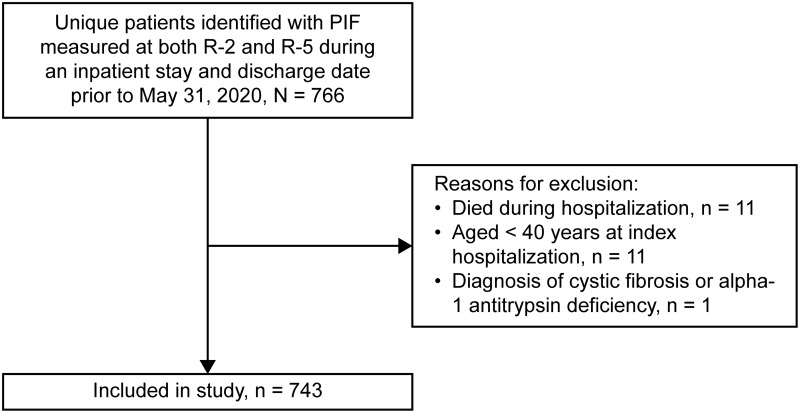
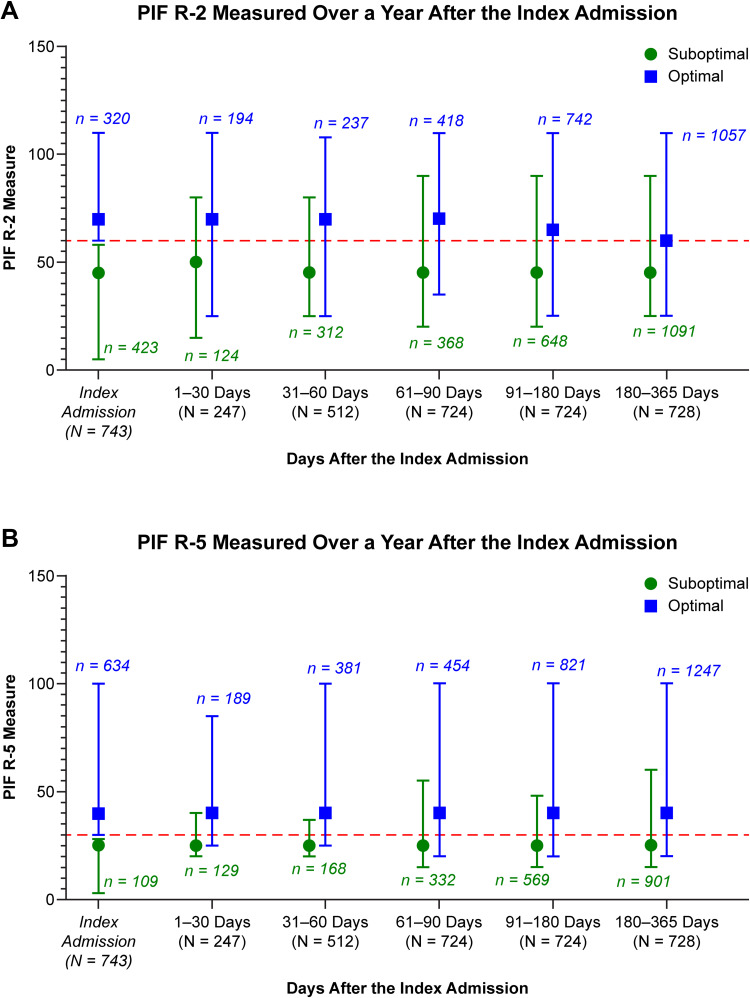
A retrospective cohort study was conducted using electronic health record data of hospitalized COPD patients in the Wake Forest Baptist Health system (01/01/2017 through 06/30/2020). Patients with a first eligible AECOPD hospitalization (index hospitalization) who were discharged before 05/31/2020 were included. PIF was measured using the In-Check DIAL™ at both medium-low resistance (R-2) and high resistance (R-5) during the index hospitalization. For R-2 and R-5, PIF was divided into low PIF (< 60 L/min; < 30 L/min) and high PIF (≥ 60 L/min; ≥ 30 L/min) groups. The primary outcome was the prevalence of low PIF. The stability of PIF after hospitalization was described. Adjusted regression models evaluated associations between low PIF and subsequent 30-day readmissions, 90-day readmissions, and HRU outcomes, including hospitalizations, emergency department visits, inpatient days, and intensive care unit (ICU) days.
In total, 743 patients with PIF measured at R-2 and R-5 during a AECOPD hospitalization were included. The prevalence of low PIF was 56.9% at R-2 and 14.7% at R-5. PIF values were relatively stable after hospitalization. Adjusted analyses showed significant increases in HRU (all-cause hospitalizations [31%], COPD hospitalizations [33%], COPD inpatient days [46%], and COPD ICU days [24%]) during the follow-up period among patients with low PIF (< 60 L/min) at R-2. The 30- and 90-day readmission risks were similar between patients with low PIF and high PIF.
Low PIF is common among patients hospitalized for AECOPD, relatively stable after hospital discharge, and associated with increased HRU.
慢性阻塞性肺疾病(COPD)患者的峰值吸气流量(PIF)可能较低,尤其是在因 COPD 急性加重(AECOPD)住院后。
描述因 AECOPD 住院的患者特征,并评估低 PIF 的发生率、住院后 PIF 的变化,以及低 PIF 与医疗保健资源利用(HRU)结局的关系。
这是一项使用维克森林浸信会健康系统(2017 年 1 月 1 日至 2020 年 6 月 30 日)电子健康记录数据进行的回顾性队列研究。纳入了首次符合条件的 AECOPD 住院(索引住院)且在 2020 年 5 月 31 日之前出院的患者。在索引住院期间,使用 In-Check DIAL™ 在中低阻力(R-2)和高阻力(R-5)下测量 PIF。对于 R-2 和 R-5,将 PIF 分为低 PIF(<60 L/min;<30 L/min)和高 PIF(≥60 L/min;≥30 L/min)组。主要结局是低 PIF 的发生率。描述了住院后 PIF 的稳定性。调整后的回归模型评估了低 PIF 与随后 30 天再入院、90 天再入院和 HRU 结局(包括住院、急诊就诊、住院天数和重症监护病房(ICU)天数)之间的关联。
共纳入了 743 例在 AECOPD 住院期间在 R-2 和 R-5 测量 PIF 的患者。R-2 时低 PIF 的发生率为 56.9%,R-5 时为 14.7%。住院后 PIF 值相对稳定。调整后的分析显示,在 R-2 时 PIF <60 L/min 的患者在随访期间 HRU(全因住院[31%]、COPD 住院[33%]、COPD 住院天数[46%]和 COPD ICU 天数[24%])显著增加。在低 PIF(<60 L/min)患者中,30 天和 90 天再入院风险在低 PIF 和高 PIF 患者之间相似。
低 PIF 在因 AECOPD 住院的患者中很常见,出院后相对稳定,与 HRU 增加有关。