Division of Infectious Diseases, Mayo Clinic, Rochester, Minnesota, USA
Division of Infectious Diseases, Emory University School of Medicine, Grady Memorial Hospital, Atlanta, Georgia, USA.
Thorax. 2023 Jun;78(6):606-616. doi: 10.1136/thoraxjnl-2022-218744. Epub 2022 Jul 6.
COVID-19 severity is correlated with granulocyte macrophage colony-stimulating factor (GM-CSF) and C reactive protein (CRP) levels. In the phase three LIVE-AIR trial, lenzilumab an anti-GM-CSF monoclonal antibody, improved the likelihood of survival without ventilation (SWOV) in COVID-19, with the greatest effect in participants having baseline CRP below a median of 79 mg/L. Herein, the utility of baseline CRP to guide lenzilumab treatment was assessed.
A subanalysis of the randomised, blinded, controlled, LIVE-AIR trial in which lenzilumab or placebo was administered on day 0 and participants were followed through Day 28.
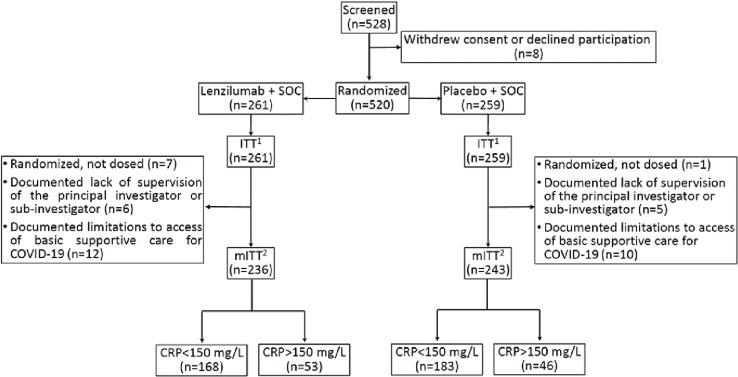
Hospitalised COVID-19 participants (N=520) with SpO2 ≤94% on room air or requiring supplemental oxygen but not invasive mechanical ventilation.
Lenzilumab (1800 mg; three divided doses, q8h, within 24 hours) or placebo infusion alongside corticosteroid and remdesivir treatments.
The primary endpoint was the time-to-event analysis difference in SWOV through day 28 between lenzilumab and placebo treatments, stratified by baseline CRP.
SWOV was achieved in 152 (90%; 95% CI 85 to 94) lenzilumab and 144 (79%; 72 to 84) placebo-treated participants with baseline CRP <150 mg/L (HR: 2.54; 95% CI 1.46 to 4.41; p=0.0009) but not with CRP ≥150 mg/L (HR: 1.04; 95% CI 0.51 to 2.14; p=0.9058). A statistically significant interaction between CRP and lenzilumab treatment was observed (p=0.044). Grade ≥3 adverse events with lenzilumab were comparable to placebo in both CRP strata. No treatment-emergent serious adverse events were attributed to lenzilumab.
Hospitalised hypoxemic patients with COVID-19 with baseline CRP <150 mg/L derived the greatest clinical benefit from treatment with lenzilumab.
NCT04351152; ClinicalTrials.gov.
COVID-19 的严重程度与粒细胞-巨噬细胞集落刺激因子(GM-CSF)和 C 反应蛋白(CRP)水平相关。在三期 LIVE-AIR 试验中,抗 GM-CSF 单克隆抗体伦齐单抗改善了 COVID-19 患者无需通气即可生存(SWOV)的可能性,在基线 CRP 中位数低于 79mg/L 的参与者中效果最大。在此,评估了基线 CRP 对伦齐单抗治疗的指导作用。
这是一项对随机、双盲、对照的 LIVE-AIR 试验的亚分析,其中在第 0 天给予伦齐单抗或安慰剂,并在第 28 天之前对参与者进行随访。
住院 COVID-19 患者(N=520),在室内空气中 SpO2≤94%或需要补充氧气但不需要有创机械通气。
伦齐单抗(1800mg;三次剂量,q8h,24 小时内)或安慰剂输注联合皮质类固醇和瑞德西韦治疗。
主要终点是通过第 28 天的时间到事件分析,比较伦齐单抗和安慰剂治疗的 SWOV,分层因素为基线 CRP。
在基线 CRP<150mg/L 的患者中,152 名(90%;95%CI 85 至 94)接受了伦齐单抗治疗,144 名(79%;72 至 84)接受了安慰剂治疗,达到了 SWOV(HR:2.54;95%CI 1.46 至 4.41;p=0.0009),而在 CRP≥150mg/L 的患者中(HR:1.04;95%CI 0.51 至 2.14;p=0.9058)则没有。在 CRP 和伦齐单抗治疗之间观察到了统计学显著的相互作用(p=0.044)。在两个 CRP 亚组中,伦齐单抗的 3 级及以上不良事件与安慰剂相当。没有因伦齐单抗治疗而出现的治疗突发严重不良事件。
基线 CRP<150mg/L 的住院低氧血症 COVID-19 患者从伦齐单抗治疗中获益最大。
NCT04351152;ClinicalTrials.gov。