Temesgen Zelalem, Burger Charles D, Baker Jason, Polk Christopher, Libertin Claudia, Kelley Colleen, Marconi Vincent C, Orenstein Robert, Durrant Cameron, Chappell Dale, Ahmed Omar, Chappell Gabrielle, Badley Andrew D
Mayo Clinic, Division of Infectious Disease, Rochester, MN.
Mayo Clinic, Division of Pulmonary, Allergy and Sleep Medicine, Jacksonville, FL.
medRxiv. 2021 May 5:2021.05.01.21256470. doi: 10.1101/2021.05.01.21256470.
Severe COVID-19 pneumonia results from a hyperinflammatory immune response (cytokine storm, CS), characterized by GM-CSF mediated activation and trafficking of myeloid cells, leading to elevation of downstream inflammatory chemokines (MCP-1, IL-8, IP-10), cytokines (IL-6, IL-1), and other markers of systemic inflammation (CRP, D-dimer, ferritin). CS leads to fever, hypotension, coagulopathy, respiratory failure, ARDS, and death. Lenzilumab is a novel Humaneered anti-human GM-CSF monoclonal antibody that directly binds GM-CSF and prevents signaling through its receptor. The LIVE-AIR Phase 3 randomized, double-blind, placebo-controlled trial investigated the efficacy and safety of lenzilumab to assess the potential for lenzilumab to improve the likelihood of ventilator-free survival (referred to herein as survival without ventilation, SWOV), beyond standard supportive care, in hospitalized subjects with severe COVID-19.
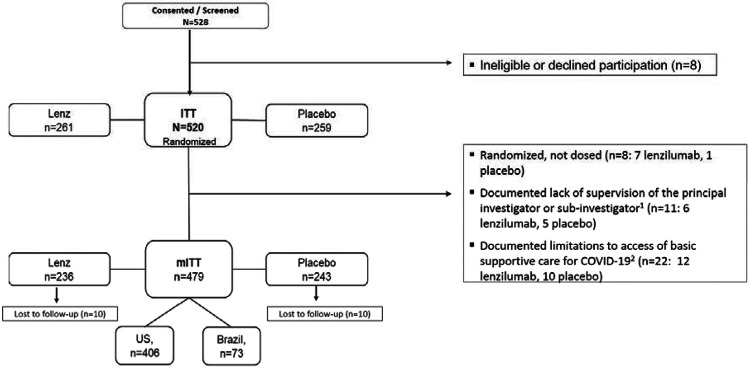
Subjects with COVID-19 (n=520), ≥18 years, and ≤94% oxygen saturation on room air and/or requiring supplemental oxygen, but not invasive mechanical ventilation, were randomized to receive lenzilumab (600 mg, n=261) or placebo (n=259) via three intravenous infusions administered 8 hours apart. Subjects were followed through Day 28 following treatment.
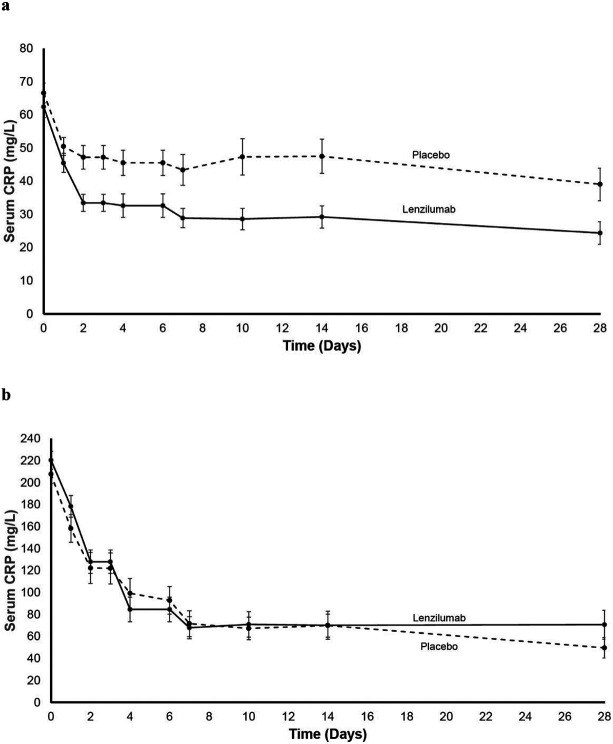
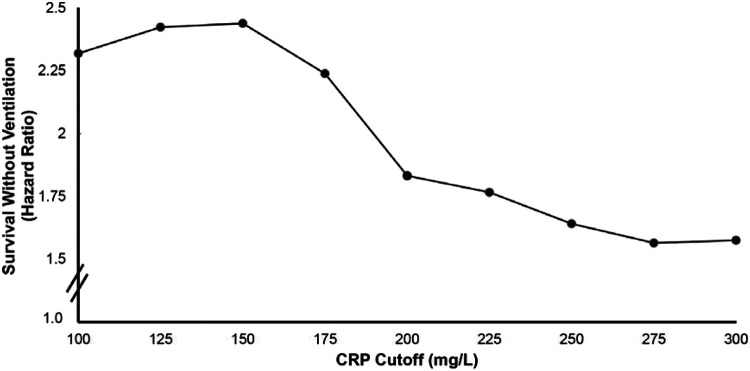
Baseline demographics were comparable between the two treatment groups: male, 64.7%; mean age, 60.5 years; mean BMI, 32.5 kg/m; mean CRP, 98.36 mg/L; CRP was <150 mg/L in 77.9% of subjects. The most common comorbidities were obesity (55.1%), diabetes (53.4%), chronic kidney disease (14.0%), and coronary artery disease (13.6%). Subjects received steroids (93.7%), remdesivir (72.4%), or both (69.1%). Lenzilumab improved the likelihood of SWOV by 54% in the mITT population (HR: 1.54; 95%CI: 1.02-2.31, p=0.041) and by 90% in the ITT population (HR: 1.90; 1.02-3.52, nominal p=0.043) compared to placebo. SWOV also relatively improved by 92% in subjects who received both corticosteroids and remdesivir (1.92; 1.20-3.07, nominal p=0.0067); by 2.96-fold in subjects with CRP<150 mg/L and age <85 years (2.96; 1.63-5.37, nominal p=0.0003); and by 88% in subjects hospitalized ≤2 days prior to randomization (1.88; 1.13-3.12, nominal p=0.015). Survival was improved by 2.17-fold in subjects with CRP<150 mg/L and age <85 years (2.17; 1.04-4.54, nominal p=0.040).
Lenzilumab significantly improved SWOV in hospitalized, hypoxic subjects with COVID-19 pneumonia over and above treatment with remdesivir and/or corticosteroids. Subjects with CRP<150 mg/L and age <85 years demonstrated an improvement in survival and had the greatest benefit from lenzilumab. NCT04351152.
重症新型冠状病毒肺炎(COVID-19)是由过度炎症性免疫反应(细胞因子风暴,CS)引起的,其特征是粒细胞-巨噬细胞集落刺激因子(GM-CSF)介导的髓样细胞活化和迁移,导致下游炎症趋化因子(单核细胞趋化蛋白-1、白细胞介素-8、干扰素诱导蛋白-10)、细胞因子(白细胞介素-6、白细胞介素-1)及其他全身炎症标志物(C反应蛋白、D-二聚体、铁蛋白)升高。细胞因子风暴会导致发热、低血压、凝血病、呼吸衰竭、急性呼吸窘迫综合征(ARDS)及死亡。伦齐单抗是一种新型人源化抗人GM-CSF单克隆抗体,可直接结合GM-CSF并阻止其通过受体进行信号传导。LIVE-AIR 3期随机、双盲、安慰剂对照试验研究了伦齐单抗在重症COVID-19住院患者中,超越标准支持治疗改善无呼吸机生存(本文称为无通气生存,SWOV)可能性的疗效和安全性。
年龄≥18岁、室内空气下氧饱和度≤94%和/或需要补充氧气但无需创机械通气的COVID-19患者(n = 520),被随机分配接受伦齐单抗(600 mg,n = 261)或安慰剂(n = 259),通过每隔8小时进行的三次静脉输注给药。治疗后对患者随访至第28天。
两个治疗组的基线人口统计学特征具有可比性:男性占64.7%;平均年龄60.5岁;平均体重指数32.5 kg/m²;平均C反应蛋白98.36 mg/L;77.9%的患者C反应蛋白<150 mg/L。最常见的合并症为肥胖(55.1%)、糖尿病(53.4%)、慢性肾脏病(14.0%)和冠状动脉疾病(13.6%)。患者接受了类固醇治疗(93.7%)、瑞德西韦治疗(72.4%)或两者联合治疗(69.1%)。与安慰剂相比,伦齐单抗使mITT人群的无通气生存可能性提高了54%(风险比:1.54;95%置信区间:1.02 - 2.31,p = 0.041),使ITT人群的无通气生存可能性提高了90%(风险比:1.90;1.02 - 3.52,名义p = 0.043)。在同时接受皮质类固醇和瑞德西韦治疗的患者中,无通气生存也相对提高了92%(1.92;1.20 - 3.07,名义p = 0.0067);在C反应蛋白<150 mg/L且年龄<85岁的患者中提高了2.96倍(2.96;1.63 - 5.37,名义p = 0.0003);在随机分组前住院≤2天的患者中提高了88%(1.88;1.13 - 3.12,名义p = 0.015)。在C反应蛋白<150 mg/L且年龄<85岁的患者中,生存改善了2.17倍(2.17;1.04 - 4.54,名义p = 0.040)。
与瑞德西韦和/或皮质类固醇治疗相比,伦齐单抗显著改善了COVID-19肺炎住院低氧患者的无通气生存。C反应蛋白<150 mg/L且年龄<85岁的患者生存得到改善,且从伦齐单抗中获益最大。NCT04351152。