Johns Hopkins Sidney Kimmel Cancer Center, Baltimore, Maryland.
Department of Internal Medicine, Johns Hopkins University Hospital, Baltimore, Maryland.
JAMA Netw Open. 2022 Jul 1;5(7):e2220543. doi: 10.1001/jamanetworkopen.2022.20543.
Disparities in access to telemedicine were identified at the onset of the COVID-19 pandemic, but the consequences of these disparities are not well characterized.
To investigate factors associated with successfully accessing and completing telemedicine visits and the association between telemedicine visit success and clinical outcomes among patients with thoracic cancer.
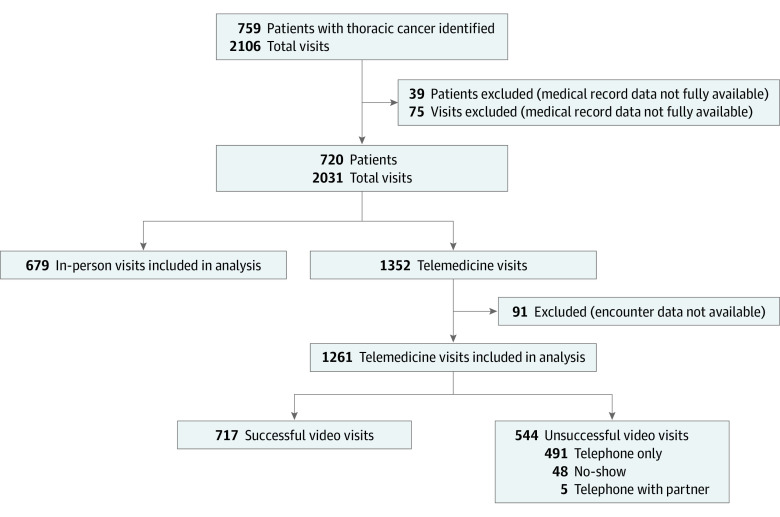
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study included patients who attended outpatient visits at the thoracic oncology division of Johns Hopkins Medical Institute in Baltimore, Maryland, from March 1 to July 17, 2020.
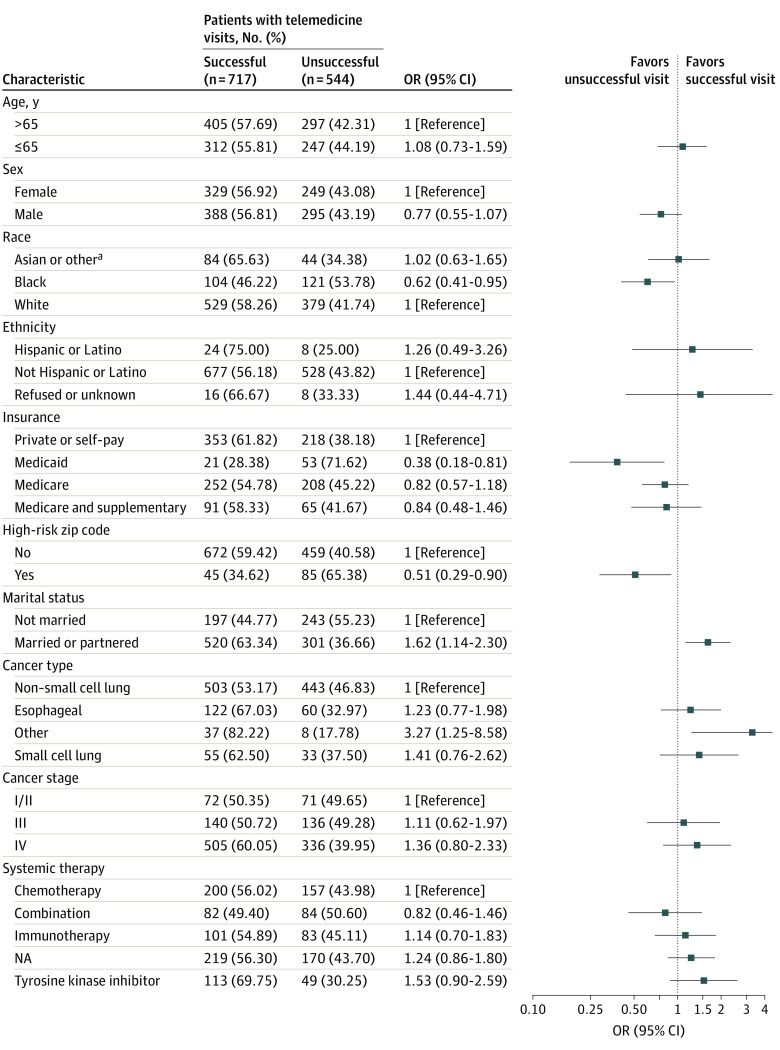
Associations of age, sex, race, ethnicity, insurance status, marital status, zip code, type of cancer, cancer stage, and type of therapy with telemedicine visit success (defined as completed visits with synchronous audio-video connection) and of visit success status with changes in therapy and odds of emergency department and urgent care visits, hospitalizations, and death were assessed using χ2 and Fisher exact tests and are reported as odds ratios (ORs).
A total of 720 patients and 1940 visits with complete data were included in the analysis; the median patient age was 65.7 years (range, 54.7-76.7 years), and 384 (53.33%) were male. Of the 1940 visits, 679 (35.00%) were in person and 1261 (65.00%) were telemedicine. Of the telemedicine visits, 717 (56.86%) were successful and 544 (43.14%) were unsuccessful. Patients who were Black (OR, 0.62; 95% CI, 0.41-0.95), had Medicaid (OR, 0.38; 95% CI, 0.18-0.81), or were from a zip code with an elevated risk of cancer mortality (OR, 0.51; 95% CI, 0.29-0.90) were less likely to have successful telemedicine visits than to have unsuccessful visits. Patients with at least 1 unsuccessful telemedicine visit had higher likelihood of an emergency department (OR, 2.73; 95% CI, 1.42-5.22) or urgent care (OR, 4.50; 95% CI, 2.41-8.41) visit or hospitalization (OR, 2.37; 95% CI, 1.17-4.80). Similarly, patients who had no successful telemedicine visits and for whom more than 1 telemedicine visit was scheduled had a higher likelihood of an emergency department (OR, 3.43; 95% CI 1.80-6.52) or urgent care (OR, 4.24; 95% CI 2.24-8.03) visit or hospitalization (OR, 4.19; 95% CI 2.17-8.10). Patients with all successful telemedicine visits (OR, 0.52; 95% CI, 0.30-0.90) or only 1, unsuccessful visit (OR, 0.32; 95% CI, 0.13-0.75) had lower odds of death compared with patients seen in-person only. Starting a new therapy was associated with lower odds of having a telemedicine visit vs an in-person visit (OR, 0.49; 95% CI, 0.37-0.64) and higher odds of a successful telemedicine visit vs an unsuccessful telemedicine visit (OR, 1.90; 95% CI, 1.28-2.82).
In this cohort study, patients with thoracic cancer who were Black, had Medicaid, or were from a zip code with a high risk of cancer mortality had increased odds of unsuccessful telemedicine visits compared with their counterparts and unsuccessful telemedicine visits were associated with worse clinical outcomes compared with successful visits. These findings suggest that more work is needed to improve telemedicine access for disadvantaged patients.
在 COVID-19 大流行开始时就发现了远程医疗获取方面的差距,但这些差距的后果尚不清楚。
调查与成功访问和完成远程医疗访问相关的因素,以及胸癌患者远程医疗访问成功率与临床结果之间的关联。
设计、地点和参与者:这项回顾性队列研究包括 2020 年 3 月 1 日至 7 月 17 日在马里兰州巴尔的摩市约翰霍普金斯医学研究所胸肿瘤科就诊的门诊患者。
使用卡方和 Fisher 精确检验评估年龄、性别、种族、民族、保险状况、婚姻状况、邮政编码、癌症类型、癌症分期和治疗类型与远程医疗访问成功率(定义为完成同步音频-视频连接的访问)的关联,以及访问成功率与治疗变化、急诊和紧急护理就诊、住院和死亡的几率之间的关联,并用比值比(OR)表示。
共纳入 720 名患者和 1940 次有完整数据的就诊;患者的中位年龄为 65.7 岁(范围,54.7-76.7 岁),384 名(53.33%)为男性。在 1940 次就诊中,679 次为面对面就诊,1261 次为远程医疗就诊。在远程医疗就诊中,717 次(56.86%)成功,544 次(43.14%)不成功。与不成功就诊相比,黑人(OR,0.62;95%CI,0.41-0.95)、有医疗补助(OR,0.38;95%CI,0.18-0.81)或来自癌症死亡率高风险邮政编码(OR,0.51;95%CI,0.29-0.90)的患者进行远程医疗就诊的成功率较低。至少有 1 次不成功远程医疗就诊的患者更有可能前往急诊(OR,2.73;95%CI,1.42-5.22)或紧急护理(OR,4.50;95%CI,2.41-8.41)就诊或住院(OR,2.37;95%CI,1.17-4.80)。同样,没有成功远程医疗就诊且计划进行多次远程医疗就诊的患者,更有可能前往急诊(OR,3.43;95%CI,1.80-6.52)或紧急护理(OR,4.24;95%CI,2.24-8.03)就诊或住院(OR,4.19;95%CI,2.17-8.10)。所有远程医疗就诊均成功(OR,0.52;95%CI,0.30-0.90)或仅 1 次不成功就诊(OR,0.32;95%CI,0.13-0.75)的患者与仅面对面就诊的患者相比,死亡几率较低。开始新的治疗与远程医疗就诊的可能性较低(OR,0.49;95%CI,0.37-0.64)和远程医疗就诊成功率较高(OR,1.90;95%CI,1.28-2.82)相关。
在这项队列研究中,与胸癌患者相比,黑人、有医疗补助或来自癌症死亡率高风险邮政编码的患者,远程医疗就诊不成功的几率较高,且不成功的远程医疗就诊与临床结果较差相关。这些发现表明,需要做更多的工作来改善弱势患者的远程医疗获取。