Department of Pediatrics, City of Hope, Duarte, California.
Department of Population Sciences, Beckman Research Institute, City of Hope, Duarte, California.
Cancer Epidemiol Biomarkers Prev. 2022 Nov 2;31(11):2004-2010. doi: 10.1158/1055-9965.EPI-21-1449.
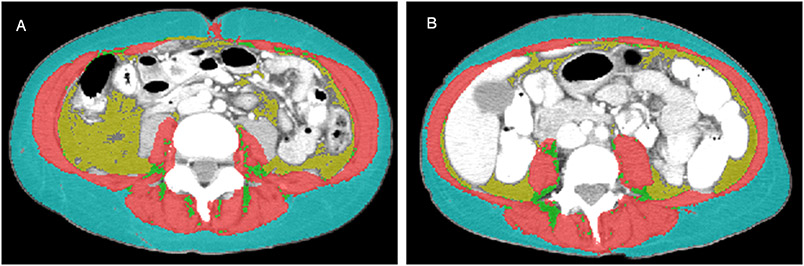
Allogeneic hematopoietic cell transplantation (HCT) recipients have increased risk of developing glucose intolerance and diabetes mellitus (DM). The strongest risk factor for glucose intolerance is being overweight/obese, as determined by body mass index (BMI), which does not account for differences in body composition. We examined the association between body composition measures from pre-HCT CT and early-onset (≤30 days) de novo glucose intolerance after HCT, and determined its impact on nonrelapse mortality (NRM).
This study included 749 patients without pre-HCT DM. Skeletal muscle loss [abnormal skeletal muscle gauge (SMG)] and abnormal visceral adiposity (VA) were defined by sex-specific tertiles. Fine-Gray proportional subdistribution HR estimates and 95% confidence intervals (CI) were obtained to determine the association between muscle loss and VA and development of glucose intolerance. 1 year NRM was calculated for patients alive at day 30.
Median age at HCT was 50.2 years. By day 30, 8.1% of patients developed glucose intolerance and 731 remained alive. In multivariable analysis, abnormal SMG was associated with increased risk of glucose intolerance in nonoverweight (BMI < 25 kg/m2) patients (HR = 3.00; 95% CI, 1.15-7.81; P = 0.024); abnormal VA was associated with increased risk of glucose intolerance in overweight/obese patients (HR = 2.26; 95% CI, 1.24-4.12; P = 0.008). Glucose intolerance was independently associated with NRM (HR = 1.88; 95% CI, 1.05-3.39; P = 0.035).
Abnormal SMG and VA were associated with glucose intolerance in nonoverweight and overweight/obese patients, respectively, which contributed to increased risk of 1 year NRM.
This information may guide personalized interventions to decrease the risk of adverse outcomes after HCT. See related commentary by Giri and Williams, p. 2002.
异基因造血细胞移植(HCT)受者发生葡萄糖耐量受损和糖尿病(DM)的风险增加。超重/肥胖是葡萄糖耐量受损的最强危险因素,这是通过体重指数(BMI)确定的,但不能反映身体成分的差异。我们研究了 HCT 前 CT 检查中身体成分测量值与 HCT 后早期(≤30 天)新发葡萄糖耐量受损之间的关系,并确定了其对非复发死亡率(NRM)的影响。
本研究纳入了 749 例无 HCT 前 DM 的患者。通过性别特异的三分位数,定义了骨骼肌减少[异常骨骼肌测量值(SMG)]和异常内脏肥胖(VA)。采用 Fine-Gray 比例亚分布 HR 估计值和 95%置信区间(CI),确定肌肉减少和 VA 与葡萄糖耐量受损的发展之间的关系。对于在第 30 天存活的患者,计算了 1 年 NRM。
HCT 时的中位年龄为 50.2 岁。在第 30 天,8.1%的患者发生葡萄糖耐量受损,731 例患者存活。多变量分析显示,非超重(BMI<25kg/m2)患者中异常 SMG 与葡萄糖耐量受损风险增加相关(HR=3.00;95%CI,1.15-7.81;P=0.024);超重/肥胖患者中异常 VA 与葡萄糖耐量受损风险增加相关(HR=2.26;95%CI,1.24-4.12;P=0.008)。葡萄糖耐量受损与 NRM 独立相关(HR=1.88;95%CI,1.05-3.39;P=0.035)。
异常 SMG 和 VA 分别与非超重和超重/肥胖患者的葡萄糖耐量受损相关,这导致 1 年 NRM 风险增加。
这些信息可能有助于指导 HCT 后降低不良结局风险的个性化干预措施。有关评论见 Giri 和 Williams 的文章,第 2002 页。