Numata Kenji, Sakurai Chinami, Mizobe Michiko, Homma Yosuke, Takahashi Jin, Funakoshi Hiraku
Emergency Department, St. Marianna University Hospital, Kawasaki, JPN.
Department of Emergency and Critical Care Medicine, Tokyobay Urayasu Ichikawa Medical Center, Urayasu, JPN.
Cureus. 2022 May 30;14(5):e25502. doi: 10.7759/cureus.25502. eCollection 2022 May.
Cardiopulmonary resuscitation (CPR) for out-of-hospital cardiac arrest (OHCA) patients during the coronavirus disease 2019 (COVID-19) pandemic carries an added risk of COVID-19 infection for healthcare workers. However, because of the shortage of medical supplies and limited evidence of COVID-19 in the initial stages of the pandemic, strategies for the management of OHCA patients may have varied across hospitals.
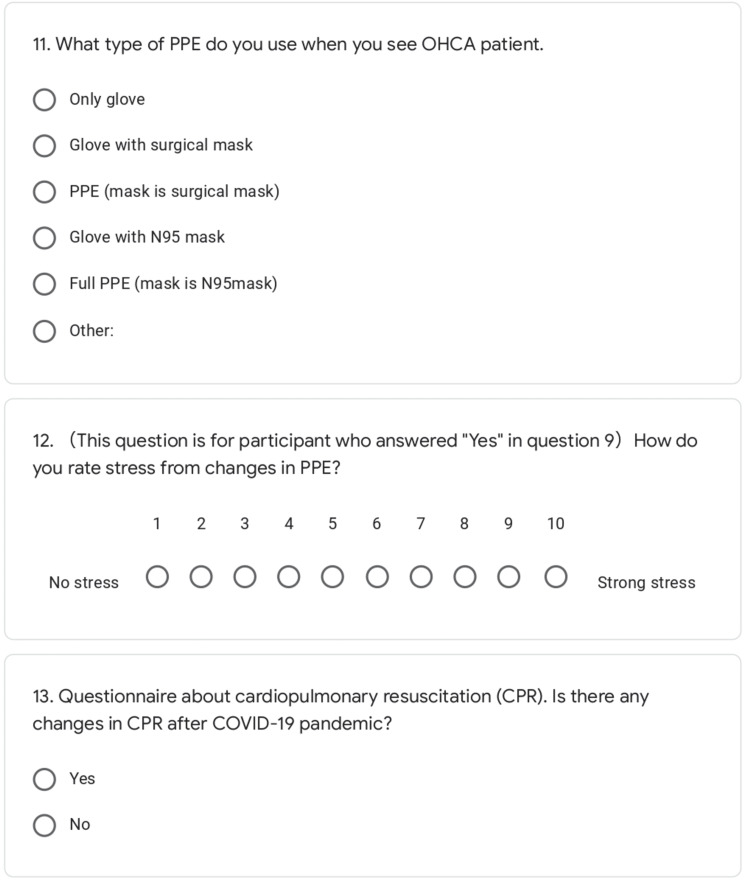
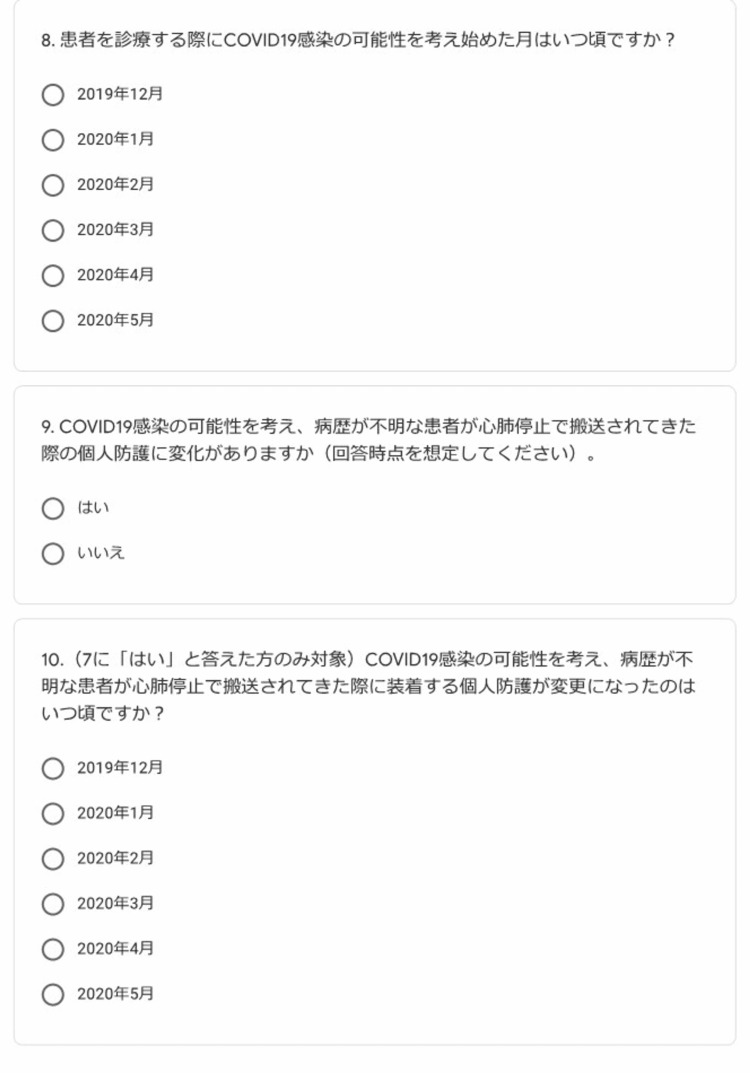
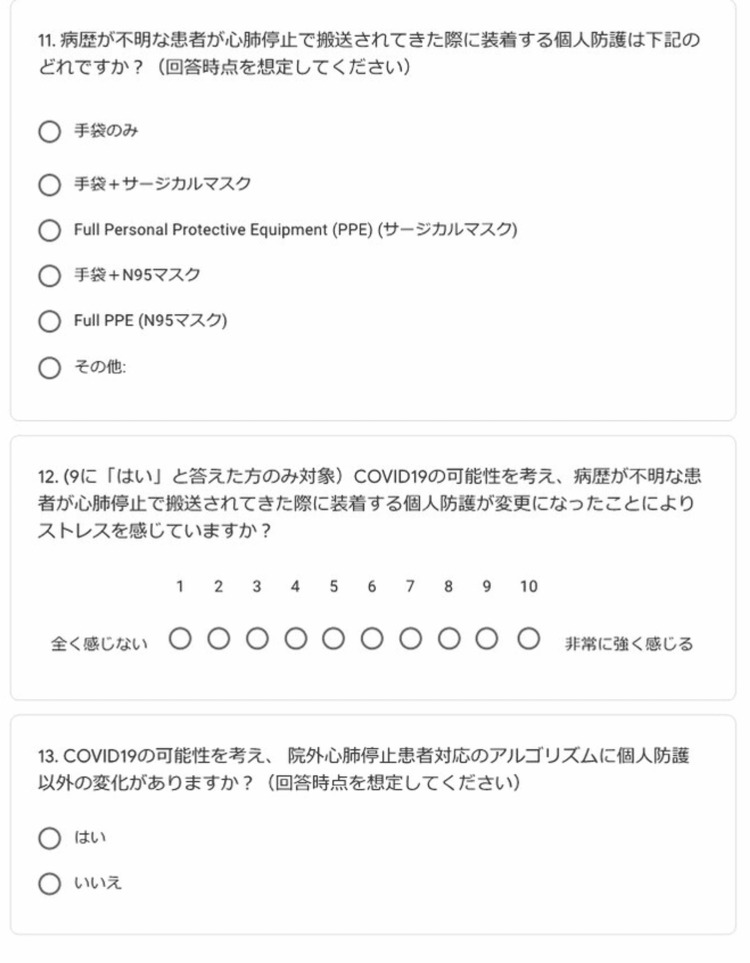
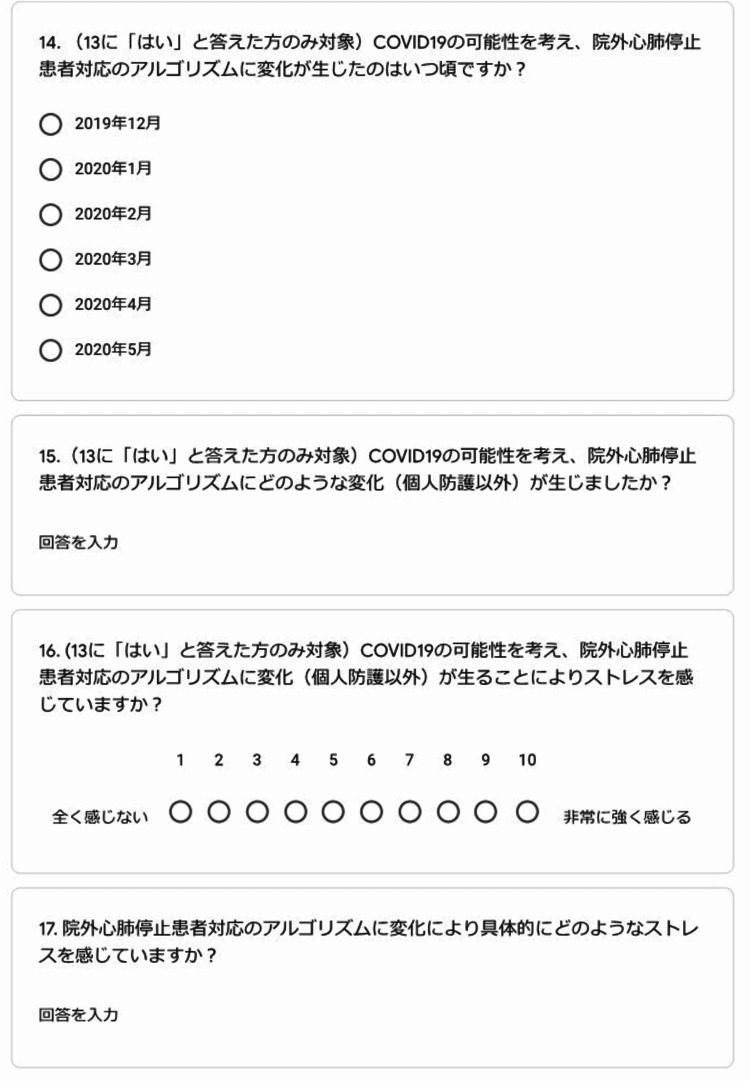
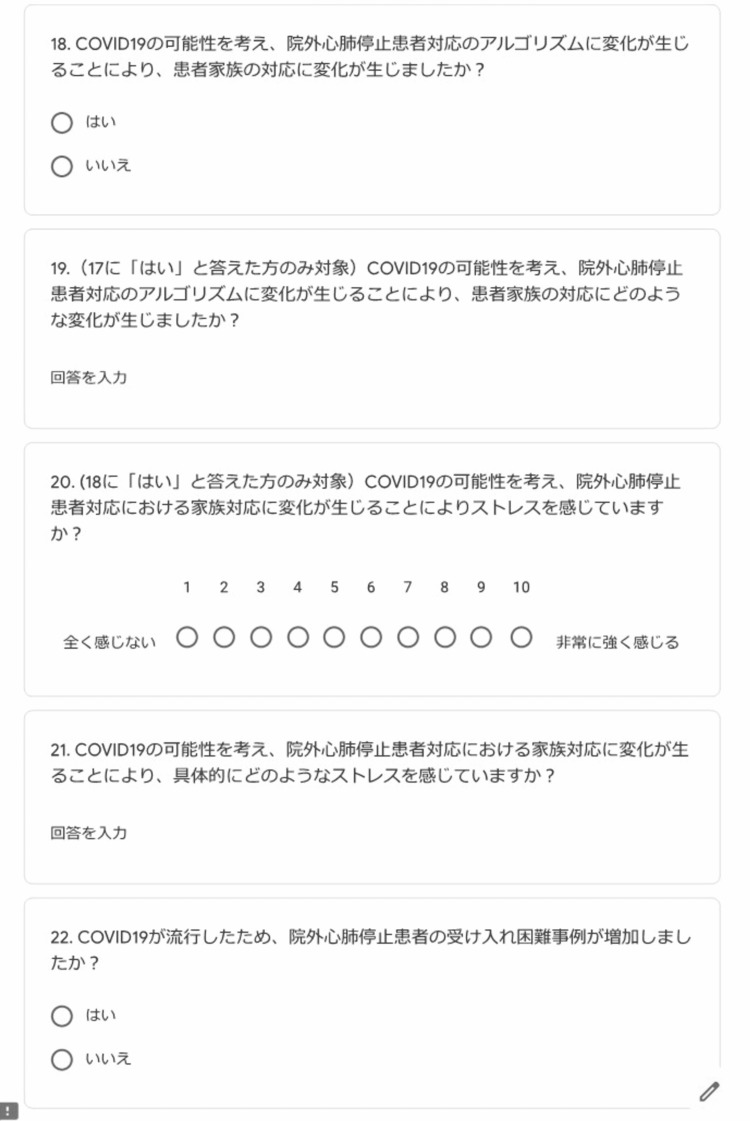
A web-based questionnaire was used. The first section collected data about physician characteristics. In the second section, participants responded "Yes" or "No," if they had made changes in the areas of "personal protective equipment (PPE)" or "CPR Algorithm" for OHCA patients (these changes were the personal views of the surveyed respondents). The questionnaire was sent to the members of the Emergency Medicine Alliance mailing list. The response period was from May 22 to June 5, 2020 (the first state of emergency related to COVID-19 was declared on April 7, 2020, in Japan). Participants were asked to indicate their stress level resulting from these changes using the Likert scale ranging from 1 to 10, where 1 = "no stress" and 10 = "severe stress."
A total of 110 physicians responded during the study period. The majority of participants reported changes in "PPE" (n = 106, 96.4%) and "CPR Algorithm" (n = 86, 78.2%). The reported stress level due to changes in PPE was 8 (IQR 6-9) and due to changes in the CPR algorithm, it was 7 (IQR 5-8).
Findings of this study suggest that physicians experienced changes in care for OHCA patients and felt stress during the initial stage of the COVID-19 pandemic. Thus, it would be better to list the actual measures that can be undertaken to prepare for any future pandemics.
在2019冠状病毒病(COVID-19)大流行期间,对院外心脏骤停(OHCA)患者进行心肺复苏(CPR)会给医护人员带来额外的COVID-19感染风险。然而,由于医疗物资短缺以及在大流行初期COVID-19的证据有限,各医院对OHCA患者的管理策略可能有所不同。
采用基于网络的问卷调查。第一部分收集有关医生特征的数据。在第二部分中,如果参与者在OHCA患者的“个人防护装备(PPE)”或“CPR算法”方面做出了改变(这些改变是被调查者的个人观点),则回答“是”或“否”。问卷发送给了急诊医学联盟邮件列表的成员。回复期为2020年5月22日至6月5日(日本于2020年4月7日宣布与COVID-19相关的首次紧急状态)。要求参与者使用从1到10的李克特量表指出这些改变所带来的压力水平,其中1表示“无压力”,10表示“严重压力”。
在研究期间共有110名医生回复。大多数参与者报告在“PPE”(n = 106,96.4%)和“CPR算法”(n = 86,78.2%)方面有改变。因PPE改变而报告的压力水平为8(四分位距6 - 9),因CPR算法改变而报告的压力水平为7(四分位距5 - 8)。
本研究结果表明,在COVID-19大流行初期,医生在OHCA患者的护理方面经历了变化并感到压力。因此,最好列出为未来任何大流行做准备时可以采取的实际措施。