Mckeon Katherine, Sibbel Scott, Brunelli Steven M, Matheson Erin, Lefeber Nick, Epps Meghan, Tentori Francesca
DaVita Clinical Research, Minneapolis, MN.
DaVita Inc, Denver, CO.
Kidney Med. 2022 May 27;4(7):100490. doi: 10.1016/j.xkme.2022.100490. eCollection 2022 Jul.
RATIONALE & OBJECTIVE: Treatment options for kidney failure are complex, and the majority of patients transitioning to dialysis lack important information about treatment options and are not prepared to make informed decisions about their care. Correspondingly, the majority of patients who start dialysis default to in-center hemodialysis using a central venous catheter for vascular access as the initial modality; furthermore, hospital admissions, mortality, and infections are exceedingly common over the first few months.
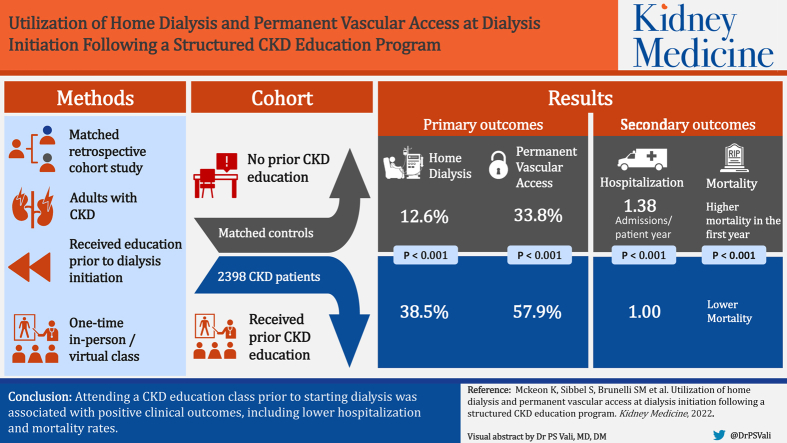
Matched retrospective cohort study.
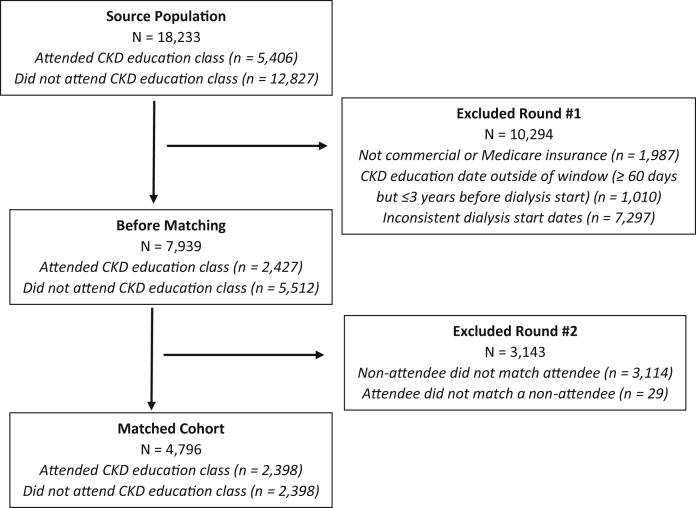
SETTING & PATIENTS: 2,398 adult patients with chronic kidney disease (CKD) who attended a structured CKD education program and pair-matched control patients who did not receive education before starting dialysis between January 2018 and June 2019.
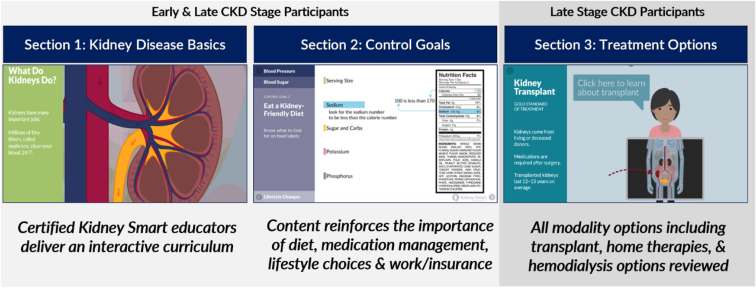
CKD education attendance documented from 2 months (60 days)-3 years before dialysis initiation. CKD education consisted of a 1-time, 90-minute, inperson or virtual class.
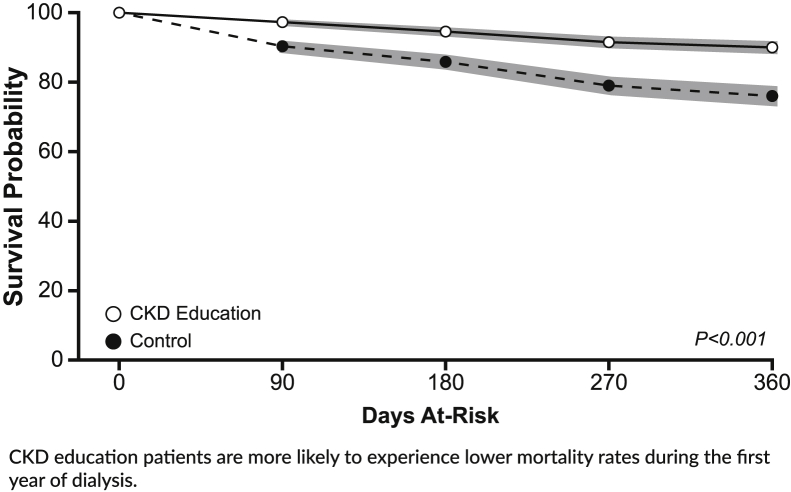
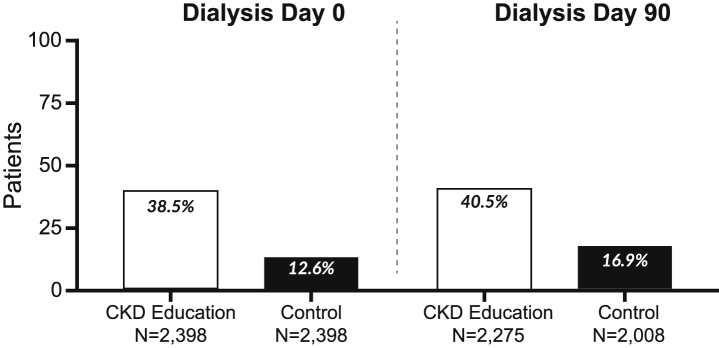
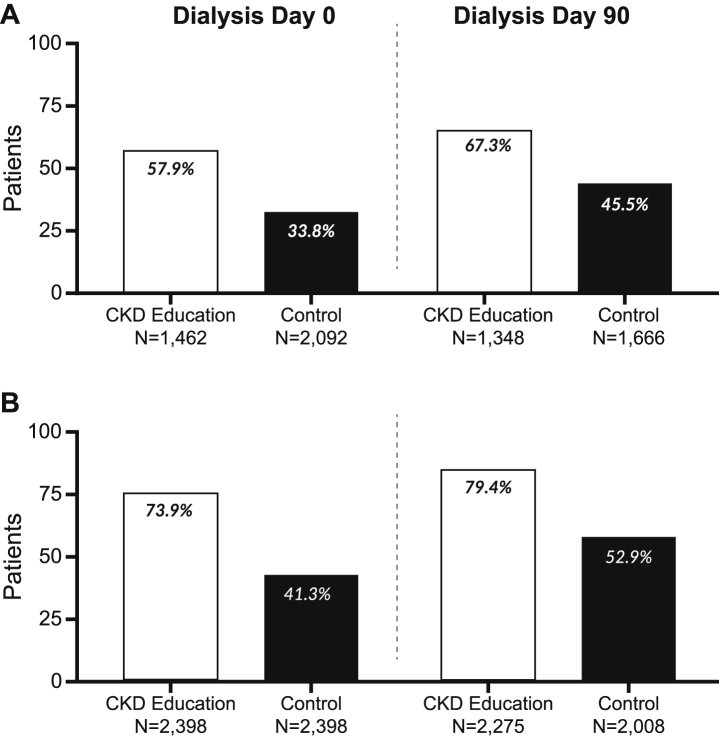
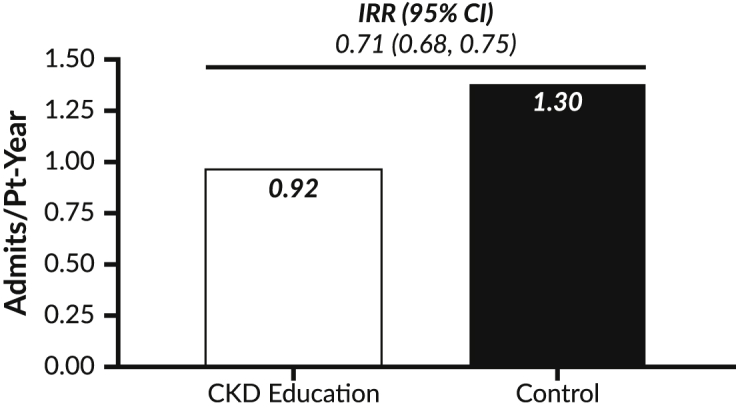
Primary outcomes were dialysis modality and vascular access type on the first day of dialysis (day 0) and at day 90 after dialysis initiation. Secondary outcomes included hospitalizations and deaths during the first year of receiving dialysis.
Generalized linear models were used to compare outcomes between patients receiving CKD education and controls.
Compared with controls, CKD education patients were more frequently receiving home dialysis (38.5% vs 12.6%, < 0.001) and used a permanent vascular access (57.9% vs 33.8%, < 0.001) at dialysis initiation; differences were minimally attenuated and remained statistically significant at day 90. Hospitalization rates were lower among CKD education patients than among controls during the first year of receiving dialysis (1.00 vs 1.38 admissions per patient-year; < 0.001). CKD education patients also had lower mortality over the first year of receiving dialysis ( < 0.001).
Bias and confounding cannot fully be accounted for in an observational study. Analyses only included patients with commercial and Medicare insurance who received CKD care before dialysis initiation and may not be generalizable to other patient populations.
Our findings indicate that attending a CKD education class before starting dialysis resulted in positive clinical outcomes, including reduction in hospitalization and mortality rates. Broad implementation of structured CKD education may result in more patients choosing home dialysis as their first treatment option and reduce the risk of adverse outcomes in the crucial early period after dialysis initiation.
肾衰竭的治疗方案复杂,大多数开始接受透析治疗的患者缺乏关于治疗方案的重要信息,并且未做好做出明智医疗决策的准备。相应地,大多数开始透析的患者默认采用中心静脉导管进行中心血液透析作为初始治疗方式;此外,在最初几个月里,住院、死亡和感染极为常见。
配对回顾性队列研究。
2398例成年慢性肾脏病(CKD)患者,这些患者参加了一个结构化的CKD教育项目,以及在2018年1月至2019年6月期间开始透析前未接受教育的配对对照患者。
在开始透析前2个月(60天)至3年期间记录的CKD教育参与情况。CKD教育包括一次时长90分钟的面对面或虚拟课程。
主要结局指标为透析第一天(第0天)和开始透析后第90天的透析方式和血管通路类型。次要结局指标包括接受透析第一年期间的住院和死亡情况。
使用广义线性模型比较接受CKD教育的患者和对照患者的结局。
与对照组相比,接受CKD教育的患者在开始透析时更频繁地接受家庭透析(38.5%对12.6%,<0.001)且使用永久性血管通路(57.9%对33.8%,<0.001);在第90天时,差异略有减弱但仍具有统计学意义。在接受透析的第一年,接受CKD教育的患者的住院率低于对照组(每位患者每年1.00次住院对1.38次住院;<0.001)。接受CKD教育的患者在接受透析的第一年死亡率也较低(<0.001)。
在观察性研究中无法完全排除偏倚和混杂因素。分析仅纳入了在开始透析前接受过CKD治疗的商业保险和医疗保险患者,可能不适用于其他患者群体情况。
我们的研究结果表明,在开始透析前参加CKD教育课程可带来积极的临床结局,包括降低住院率和死亡率。广泛实施结构化的CKD教育可能会使更多患者选择家庭透析作为首选治疗方案,并降低透析开始后关键早期不良结局的风险。