Méndez-Bailón Manuel, Lorenzo-Villalba Noel, Romero-Correa Miriam, Josa-Laorden Claudia, Inglada-Galiana Luis, Menor-Campos Eva, Gómez-Aguirre Noelia, Clemente-Sarasa Carolina, Salas-Campos Rosario, García-Redecillas Carmen, Asenjo-Martínez María, Trullàs Joan Carles, Cortés-Rodríguez Begoña, de la Guerra-Acebal Carla, Serrado Iglesias Ana, Aparicio-Santos Reyes, Formiga Francesc, Andrès Emmanuel, Aramburu-Bodas Oscar, Salamanca-Bautista Prado
Servicio de Medicina Interna, Hospital Clínico Universitario San Carlos, Universidad Complutense de Madrid Instituto de Investigación Sanitaria (IdISSC), 28040 Madrid, Spain.
Service de Médecine Interne, Diabète et Maladies Métaboliques, Hôpitaux Universitaires de Strasbourg, 67000 Strasbourg, France.
J Clin Med. 2022 Jun 27;11(13):3709. doi: 10.3390/jcm11133709.
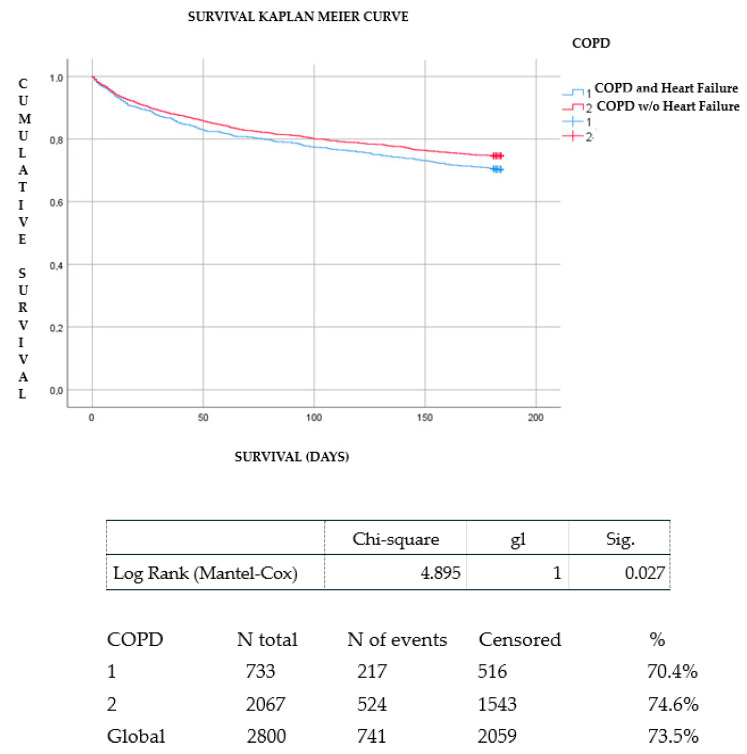
Introduction: There are studies that evaluate the association between chronic obstructive pulmonary disease (COPD) and heart failure (HF) but there is little evidence regarding the prognosis of this comorbidity in older patients admitted for acute HF. In addition, little attention has been given to the extracardiac and extrapulmonary symptoms presented by patients with HF and COPD in more advanced stages. The aim of this study was to evaluate the prognostic impact of COPD on mortality in elderly patients with acute and advanced HF and the clinical manifestations and management from a palliative point of view. Methods: The EPICTER study (“Epidemiological survey of advanced heart failure”) is a cross-sectional, multicenter project that consecutively collected patients admitted for HF in 74 Spanish hospitals. Demographic, clinical, treatment, organ-dependent terminal criteria (NYHA III-IV, LVEF <20%, intractable angina, HF despite optimal treatment), and general terminal criteria (estimated survival <6 months, patient/family acceptance of palliative approach, and one of the following: evidence of HF progression, multiple Emergency Room visits or admissions in the last six months, 10% weight loss in the last six months, and functional impairment) were collected. Terminal HF was considered if the patient met at least one organ-dependent criterion and all the general criteria. Both groups (HF with COPD and without COPD) were compared. A Kaplan−Meier survival analysis was performed to evaluate the presence of COPD on the vital prognosis of patients with HF. Results: A total of 3100 patients were included of which 812 had COPD. In the COPD group, dyspnea and anxiety were more frequently observed (86.2% vs. 75.3%, p = 0.001 and 35.4% vs. 31.2%, p = 0.043, respectively). In patients with a history of COPD, presentation of HF was in the form of acute pulmonary edema (21% vs. 14.4% in patients without COPD, p = 0.0001). Patients with COPD more frequently suffered from advanced HF (28.9% vs. 19.4%; p < 0.001). Consultation with the hospital palliative care service during admission was more frequent when patients with HF presented with associated COPD (94% vs. 6.8%; p = 0.036). In-hospital and six-month follow-up mortality was 36.5% in patients with COPD vs. 30.7% in patients without COPD, p = 0.005. The mean number of hospital admissions during follow-up was higher in patients with HF and COPD than in those with isolated HF (0.63 ± 0.98 vs. 0.51 ± 0.84; p < 0.002). Survival analysis showed that patients with a history of COPD had fewer survival days during follow-up than those without COPD (log Rank chi-squared 4.895 and p = 0.027). Conclusions: patients with HF and COPD had more severe symptoms (dyspnea and anxiety) and also a worse prognosis than patients without COPD. However, the prognosis of patients admitted to our setting is poor and many patients with HF and COPD may not receive the assessment and palliative care support they need. Palliative care is necessary in chronic non-oncologic diseases, especially in multipathologic and symptom-intensive patients. This is a clinical care aspect to be improved and evaluated in future research studies.
有研究评估了慢性阻塞性肺疾病(COPD)与心力衰竭(HF)之间的关联,但关于因急性心力衰竭入院的老年患者中这种合并症的预后,证据很少。此外,对于HF和COPD晚期患者出现的心脏外和肺外症状关注较少。本研究的目的是从姑息治疗的角度评估COPD对急性和晚期HF老年患者死亡率的预后影响以及临床表现和管理。方法:EPICTER研究(“晚期心力衰竭的流行病学调查”)是一个横断面、多中心项目,连续收集了西班牙74家医院因HF入院的患者。收集了人口统计学、临床、治疗、器官依赖终末期标准(纽约心脏协会III-IV级、左心室射血分数<20%、顽固性心绞痛、尽管进行了最佳治疗仍有HF)和一般终末期标准(估计生存期<6个月、患者/家属接受姑息治疗方法,以及以下之一:HF进展的证据、过去六个月多次急诊就诊或住院、过去六个月体重减轻10%、功能障碍)。如果患者至少符合一项器官依赖标准和所有一般标准,则视为终末期HF。对两组(合并COPD的HF和未合并COPD的HF)进行比较。进行Kaplan-Meier生存分析以评估COPD对HF患者生命预后的影响。结果:共纳入3100例患者,其中812例患有COPD。在COPD组中,更频繁观察到呼吸困难和焦虑(分别为86.2%对75.3%,p = 0.001和35.4%对31.2%,p = 0.043)。有COPD病史的患者,HF的表现形式为急性肺水肿(21%对无COPD患者的14.4%,p = 0.0001)。合并COPD的患者更常患有晚期HF(28.9%对19.4%;p < 0.001)。当HF患者合并COPD时,入院期间与医院姑息治疗服务的会诊更频繁(94%对6.8%;p = 0.036)。合并COPD患者的院内和六个月随访死亡率为36.5%,而未合并COPD患者为30.7%,p = 0.005。随访期间合并HF和COPD患者的平均住院次数高于单纯HF患者(0.63±0.98对0.51±0.84;p < 0.002)。生存分析表明,有COPD病史的患者随访期间的生存天数少于无COPD的患者(对数秩卡方值4.895,p = 0.027)。结论:合并HF和COPD的患者比未合并COPD的患者有更严重的症状(呼吸困难和焦虑),预后也更差。然而,在我们的研究环境中入院患者的预后很差,许多合并HF和COPD的患者可能没有得到他们所需的评估和姑息治疗支持。姑息治疗在慢性非肿瘤性疾病中是必要的,尤其是在多病理和症状严重的患者中。这是一个在未来研究中有待改进和评估的临床护理方面。