SAR Laboratories, Sandra Rotman Centre for Global Health, University Health Network-Toronto General Hospital, Toronto, Canada.
Department of Medicine, Division of Critical Care Medicine, Robarts Research Institute, University of Western Ontario, London, Ontario, Canada.
PLoS Med. 2022 Jul 13;19(7):e1004057. doi: 10.1371/journal.pmed.1004057. eCollection 2022 Jul.
Despite the global burden of pneumonia, reliable triage tools to identify children in low-resource settings at risk of severe and fatal respiratory tract infection are lacking. This study assessed the ability of circulating host markers of immune and endothelial activation quantified at presentation, relative to currently used clinical measures of disease severity, to identify children with pneumonia who are at risk of death.
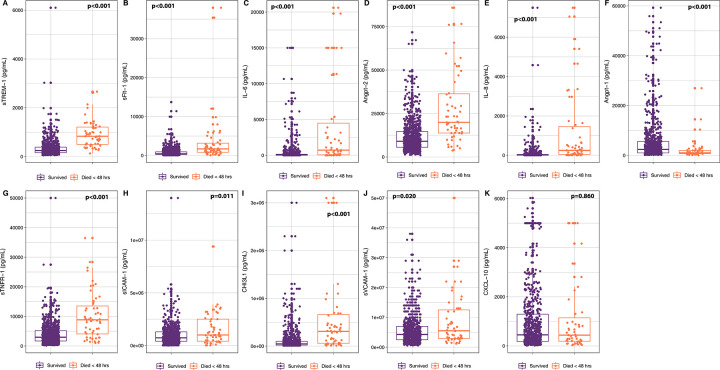
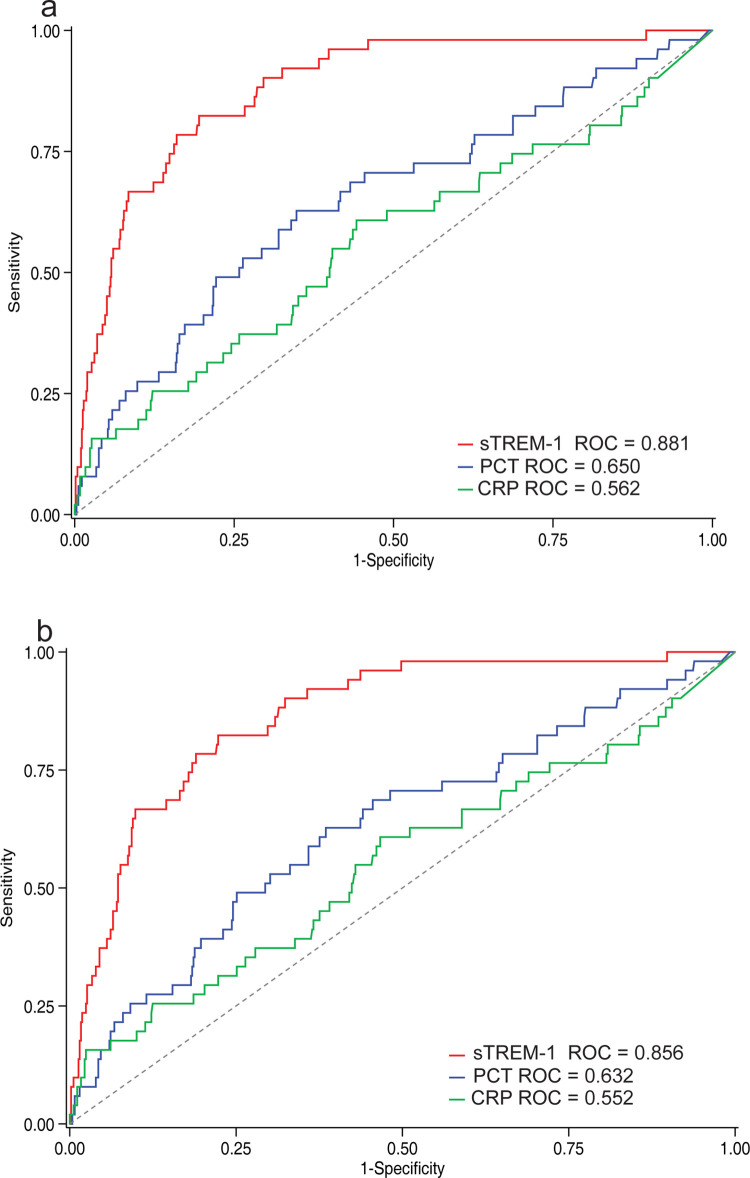
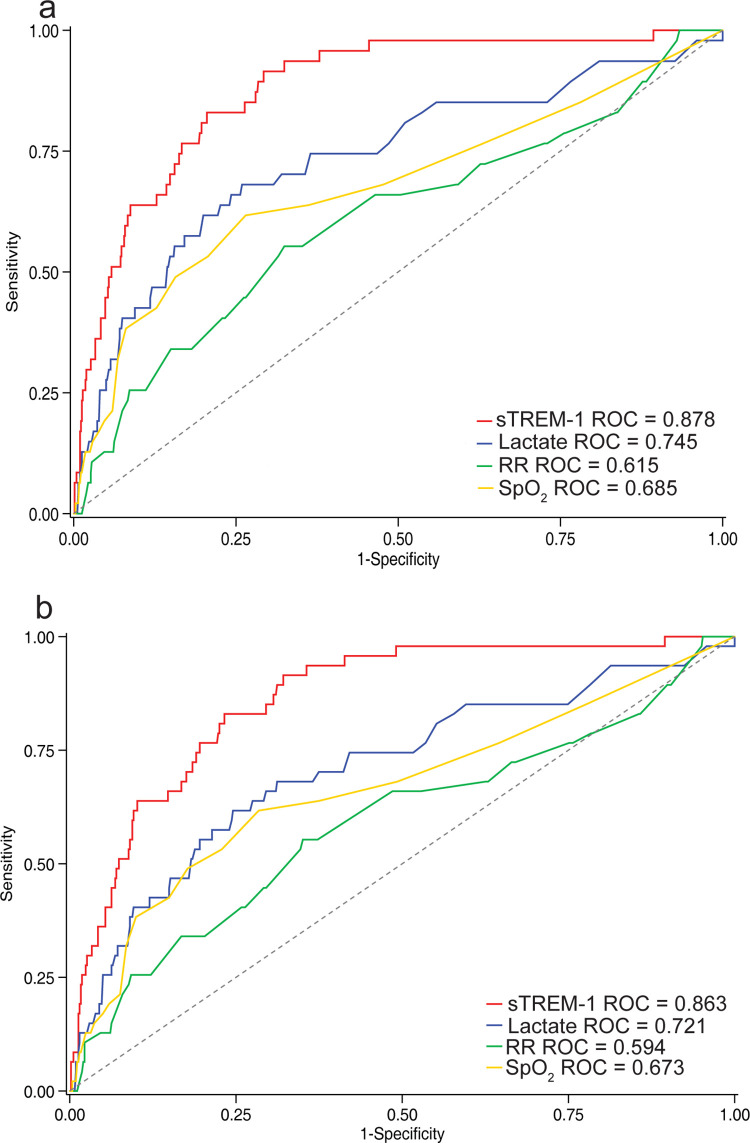
We conducted a secondary analysis of a prospective cohort study of children aged 2 to 59 months presenting to the Jinja Regional Hospital in Jinja, Uganda between February 2012 and August 2013, who met the Integrated Management of Childhood Illness (IMCI) diagnostic criteria for pneumonia. Circulating plasma markers of immune (IL-6, IL-8, CXCL-10/IP-10, CHI3L1, sTNFR1, and sTREM-1) and endothelial (sVCAM-1, sICAM-1, Angpt-1, Angpt-2, and sFlt-1) activation measured at hospital presentation were compared to lactate, respiratory rate, oxygen saturation, procalcitonin (PCT), and C-reactive protein (CRP) with a primary outcome of predicting 48-hour mortality. Of 805 children with IMCI pneumonia, 616 had severe pneumonia. Compared to 10 other immune and endothelial activation markers, sTREM-1 levels at presentation had the best predictive accuracy in identifying 48-hour mortality for children with pneumonia (AUROC 0.885, 95% CI 0.841 to 0.928; p = 0.03 to p < 0.001) and severe pneumonia (AUROC 0.870, 95% CI 0.824 to 0.916; p = 0.04 to p < 0.001). sTREM-1 was more strongly associated with 48-hour mortality than lactate (AUROC 0.745, 95% CI 0.664 to 0.826; p < 0.001), respiratory rate (AUROC 0.615, 95% CI 0.528 to 0.702; p < 0.001), oxygen saturation (AUROC 0.685, 95% CI 0.594 to 0.776; p = 0.002), PCT (AUROC 0.650, 95% CI 0.566 to 0.734; p < 0.001), and CRP (AUROC 0.562, 95% CI 0.472 to 0.653; p < 0.001) in cases of pneumonia and severe pneumonia. The main limitation of this study was the unavailability of radiographic imaging.
In this cohort of Ugandan children, sTREM-1 measured at hospital presentation was a significantly better indicator of 48-hour mortality risk than other common approaches to risk stratify children with pneumonia. Measuring sTREM-1 at clinical presentation may improve the early triage, management, and outcome of children with pneumonia at risk of death.
The trial was registered at clinicaltrial.gov (NCT04726826).
尽管肺炎在全球范围内造成了沉重负担,但仍缺乏可靠的工具来识别资源匮乏环境中发生严重和致命性下呼吸道感染的儿童。本研究评估了在就诊时量化的循环宿主免疫和内皮激活标志物,与目前用于评估疾病严重程度的临床指标相比,用于识别有死亡风险的肺炎儿童的能力。
我们对 2012 年 2 月至 2013 年 8 月期间在乌干达金贾地区医院就诊的年龄在 2 至 59 个月之间、符合儿童综合管理(IMCI)肺炎诊断标准的儿童进行了一项前瞻性队列研究的二次分析。在就诊时测量的循环血浆免疫(IL-6、IL-8、CXCL-10/IP-10、CHI3L1、sTNFR1 和 sTREM-1)和内皮(sVCAM-1、sICAM-1、Angpt-1、Angpt-2 和 sFlt-1)激活标志物与乳酸、呼吸频率、氧饱和度、降钙素原(PCT)和 C 反应蛋白(CRP)进行了比较,主要结局是预测 48 小时死亡率。在 805 名患有 IMCI 肺炎的儿童中,有 616 名患有严重肺炎。与其他 10 种免疫和内皮激活标志物相比,sTREM-1 水平在识别肺炎儿童 48 小时死亡率方面具有最佳的预测准确性(AUROC 0.885,95%CI 0.841 至 0.928;p = 0.03 至 p < 0.001)和严重肺炎(AUROC 0.870,95%CI 0.824 至 0.916;p = 0.04 至 p < 0.001)。sTREM-1 与 48 小时死亡率的相关性强于乳酸(AUROC 0.745,95%CI 0.664 至 0.826;p < 0.001)、呼吸频率(AUROC 0.615,95%CI 0.528 至 0.702;p < 0.001)、氧饱和度(AUROC 0.685,95%CI 0.594 至 0.776;p = 0.002)、PCT(AUROC 0.650,95%CI 0.566 至 0.734;p < 0.001)和 CRP(AUROC 0.562,95%CI 0.472 至 0.653;p < 0.001),用于肺炎和严重肺炎病例。本研究的主要局限性是缺乏影像学检查。
在本队列中,就诊时测量的 sTREM-1 是预测肺炎儿童 48 小时死亡率风险的显著更好指标,优于其他用于对肺炎儿童进行风险分层的常用方法。在就诊时测量 sTREM-1 可能会改善有死亡风险的肺炎儿童的早期分诊、管理和预后。
该试验在 clinicaltrial.gov(NCT04726826)上注册。