Smith Kenneth J, Wateska Angela R, Nowalk Mary Patricia, Lin Chyongchiou J, Harrison Lee H, Schaffner William, Zimmerman Richard K
School of Medicine, University of Pittsburgh, 200 Meyran Ave, Suite 200, Pittsburgh, PA, 15213, USA.
The Ohio State University College of Nursing, Columbus, OH, USA.
Infect Dis Ther. 2022 Aug;11(4):1683-1693. doi: 10.1007/s40121-022-00669-x. Epub 2022 Jul 13.
US pneumococcal vaccination recommendations for adults aged 65 years or older recently changed, with options for either 20-valent pneumococcal conjugate vaccine (PCV20) or the combination of 15-valent conjugate vaccine (PCV15) followed by 23-valent polysaccharide vaccine (PPSV23) 1 year later. Underserved minority adults are at higher risk for pneumococcal disease.
A Markov decision analysis model estimated the incremental cost-effectiveness of the newly adopted general population pneumococcal vaccination strategies in older underserved minority adults. The model examined hypothetical 65-year-old US Black cohorts (serving as a proxy for underserved minorities) and non-Black cohorts receiving PCV20 or PCV15/PPSV23, or no vaccination. Main outcome measures included incremental cost-effectiveness per quality-adjusted life year (QALY) gained and pneumococcal disease public health outcomes.
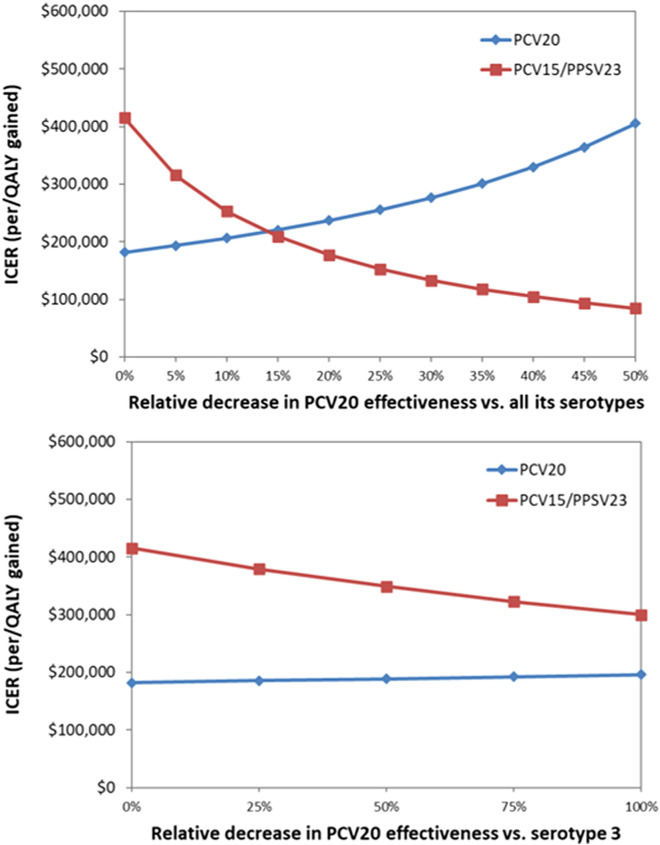
Black cohorts had a greater risk of pneumococcal disease hospitalization compared to non-Black cohorts. In Black cohorts, total per person PCV20 strategy costs, compared to no vaccination, were $124 higher while gaining 0.00073 QALY, or $169,540/QALY gained. PCV15/PPSV23 cost $535,797/QALY compared to PCV20. In the non-Black cohort, PCV20 cost $210,529/QALY gained compared to no vaccination and PCV15/PPSV23 cost $728,423/QALY. Plausible variation of vaccine effectiveness minimally affected PCV20 strategy results and made PCV15/PPSV23 more unfavorable. In scenarios where the simpler one-vaccine PCV20 strategy increased absolute vaccine uptake by 10%, PCV20 cost-effectiveness changed minimally while PCV15/PPSV23 cost in excess of $6 million/QALY in the Black cohort. In probabilistic sensitivity analyses that varied all parameters simultaneously, PCV15/PPSV23 was unlikely to be favored at thresholds less than $500,000/QALY gained.
General population recommendations for PCV20 use are substantially more economically reasonable in Black and non-Black older adult populations than PCV15/PPSV23. If using a single vaccine increases uptake, which is potentially more likely in the underserved, then PCV20 use becomes even more favorable.
美国针对65岁及以上成年人的肺炎球菌疫苗接种建议最近有所变化,有两种选择,即接种20价肺炎球菌结合疫苗(PCV20),或先接种15价结合疫苗(PCV15),一年后再接种23价多糖疫苗(PPSV23)。医疗服务不足的少数族裔成年人患肺炎球菌疾病的风险更高。
马尔可夫决策分析模型估计了新采用的针对医疗服务不足的老年少数族裔成年人的一般人群肺炎球菌疫苗接种策略的增量成本效益。该模型研究了假设的65岁美国黑人队列(作为医疗服务不足的少数族裔的代表)以及接受PCV20或PCV15/PPSV23接种或未接种疫苗的非黑人队列。主要结局指标包括每获得一个质量调整生命年(QALY)的增量成本效益以及肺炎球菌疾病的公共卫生结局。
与非黑人队列相比,黑人队列因肺炎球菌疾病住院的风险更高。在黑人队列中,与未接种疫苗相比,每人PCV20策略的总成本高出124美元,同时获得0.00073个QALY,即每获得一个QALY成本为169,540美元。与PCV20相比,PCV15/PPSV23每获得一个QALY的成本为535,797美元。在非黑人队列中,与未接种疫苗相比,PCV20每获得一个QALY的成本为210,529美元,PCV15/PPSV23每获得一个QALY的成本为728,423美元。疫苗效力的合理变化对PCV20策略结果的影响最小,而使PCV15/PPSV23更不利。在较简单的单疫苗PCV20策略使绝对疫苗接种率提高10%的情况下,PCV20的成本效益变化最小,而在黑人队列中,PCV15/PPSV23每获得一个QALY的成本超过600万美元。在同时改变所有参数的概率敏感性分析中,在每获得一个QALY成本低于500,000美元的阈值下,PCV15/PPSV23不太可能受到青睐。
在黑人和非黑人老年人群体中,针对一般人群使用PCV20的建议在经济上比PCV15/PPSV23更合理。如果使用单一疫苗能提高接种率,而这在医疗服务不足的人群中可能更有可能实现,那么使用PCV20就更具优势。