Wateska Angela R, Nowalk Mary Patricia, Altawalbeh Shoroq M, Lin Chyongchiou J, Harrison Lee H, Schaffner William, Zimmerman Richard K, Smith Kenneth J
Departments of Medicine and Family Medicine, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, USA.
Jordan University of Science and Technology, Faculty of Pharmacy, Irbid, Jordan.
J Am Geriatr Soc. 2024 Aug;72(8):2423-2433. doi: 10.1111/jgs.19031. Epub 2024 Jun 1.
Multiple factors, such as less complex U.S. adult pneumococcal recommendations that could increase vaccination rates, childhood pneumococcal vaccination indirect effects that decrease adult vaccination impact, and increased vaccine hesitancy (particularly in underserved minorities), could diminish the cost-effectiveness of programs to increase pneumococcal vaccination in older adults. Prior analyses supported the economic favorability of these programs.
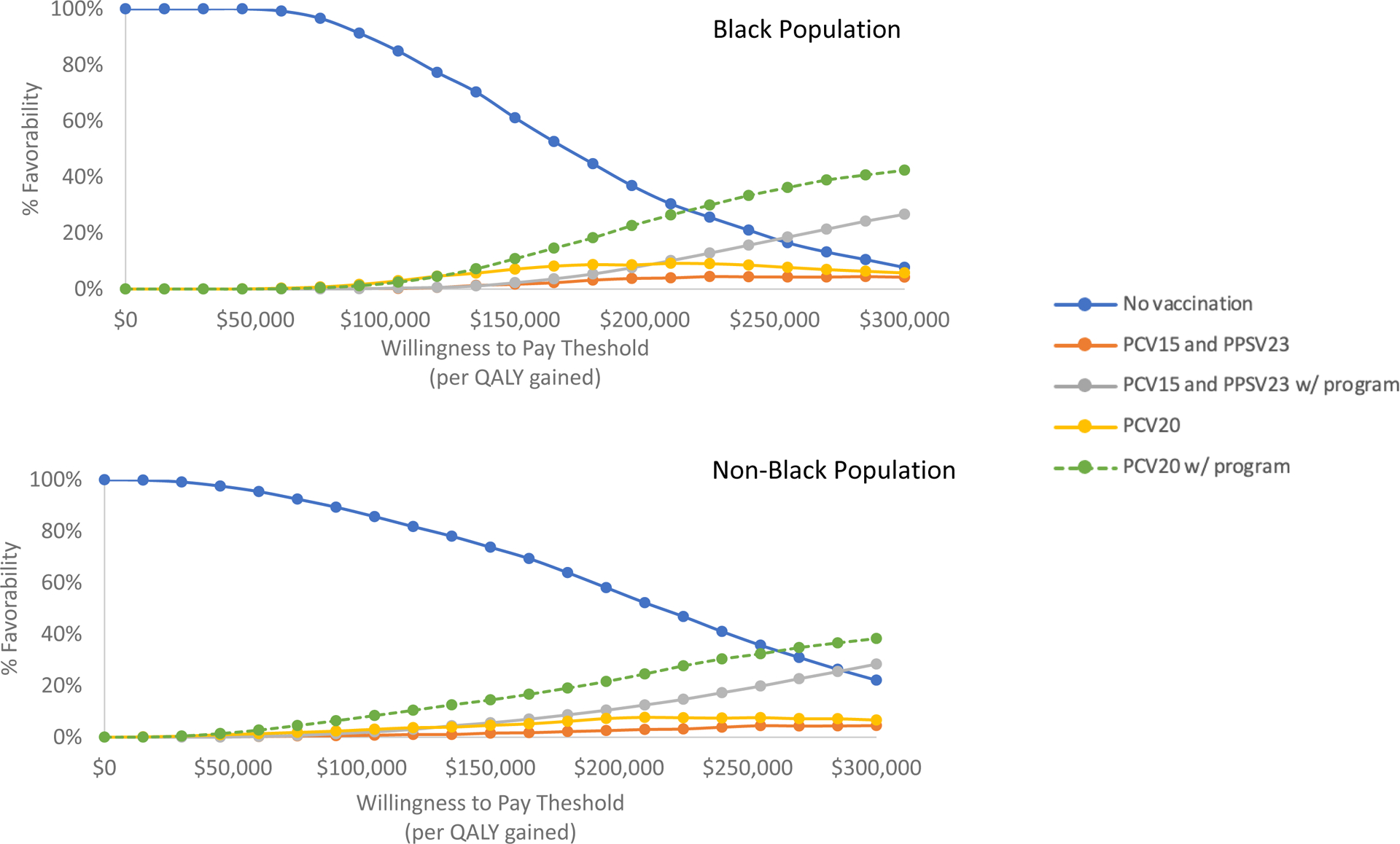
A Markov model compared no vaccination and current recommendations (either 20-valent pneumococcal conjugate vaccine [PCV20] alone or 15-valent pneumococcal conjugate vaccine plus the 23-valent pneumococcal polysaccharide vaccine [PCV15/PPSV23]) without or with programs to increase vaccine uptake in Black and non-Black 65-year-old cohorts. Pre-pandemic population- and serotype-specific pneumococcal disease risk and illness/vaccine costs came from U.S.
Program costs were $2.19 per vaccine-eligible person and increased absolute vaccination likelihood by 7.5%. Delphi panel estimates and trial data informed vaccine effectiveness values. Analyses took a healthcare perspective, discounting at 3%/year over a lifetime time horizon.
Uptake programs decreased pneumococcal disease overall. In Black cohorts, PCV20 without program cost $216,805 per quality-adjusted life year (QALY) gained compared with no vaccination; incremental cost-effectiveness was $245,546/QALY for PCV20 with program and $425,264/QALY for PCV15/PPSV23 with program. In non-Black cohorts, all strategies cost >$200,000/QALY gained. When considering the potential indirect effects from childhood vaccination, all strategies became less economically attractive. Increased vaccination with less complex strategies had negligible effects. In probabilistic sensitivity analyses, current recommendations with or without programs were unlikely to be favored at thresholds <$200,000/QALY gained.
Current U.S. pneumococcal vaccination recommendations for older adults were unlikely to be economically reasonable with or without programs to increase vaccine uptake. Alternatives to current pneumococcal vaccines that include pneumococcal serotypes associated with adult disease should be considered.
多种因素可能会降低提高老年人肺炎球菌疫苗接种率项目的成本效益,比如美国成人肺炎球菌疫苗接种建议不够复杂,本可提高接种率;儿童肺炎球菌疫苗接种的间接影响降低了成人疫苗接种效果;疫苗犹豫现象增加(尤其是在服务不足的少数群体中)。先前的分析支持这些项目在经济上的可行性。
采用马尔可夫模型,比较了不接种疫苗和当前接种建议(单独使用20价肺炎球菌结合疫苗[PCV20]或15价肺炎球菌结合疫苗加23价肺炎球菌多糖疫苗[PCV15/PPSV23])的情况,接种对象为65岁的黑人和非黑人队列,分为有无提高疫苗接种率项目两种情况。疫情前特定人群和血清型的肺炎球菌疾病风险以及疾病/疫苗成本数据来自美国。
项目成本为每位符合疫苗接种条件的人2.19美元,绝对接种可能性提高了7.5%。德尔菲专家小组的估计和试验数据为疫苗有效性值提供了依据。分析采用医疗保健视角,在终身时间范围内按每年3%进行贴现。
提高接种率项目总体上降低了肺炎球菌疾病的发生。在黑人队列中,不采用项目时,每获得一个质量调整生命年(QALY),PCV20的成本为216,805美元,与不接种疫苗相比;采用项目时,PCV20的增量成本效益比为245,546美元/QALY,PCV15/PPSV23采用项目时为425,264美元/QALY。在非黑人队列中,所有策略每获得一个QALY的成本均超过200,000美元。考虑到儿童疫苗接种的潜在间接影响后,所有策略在经济上的吸引力都降低了。采用不太复杂的策略增加疫苗接种的效果可忽略不计。在概率敏感性分析中,无论有无项目,当前的接种建议在每获得一个QALY的成本阈值低于200,000美元时都不太可能受到青睐。
无论有无提高疫苗接种率的项目,美国目前针对老年人的肺炎球菌疫苗接种建议在经济上可能都不合理。应考虑替代当前肺炎球菌疫苗的方案,这些方案应包含与成人疾病相关的肺炎球菌血清型。