Cardiothoracic Intensive Care Unit, Hôpital Marie Lannelongue, 133 avenue de la Résistance, 92350, Le Plessis Robinson, France.
School of Medicine, Paris-Saclay University, Kremlin-Bicêtre, France.
Crit Care. 2022 Jul 13;26(1):214. doi: 10.1186/s13054-022-04084-z.
The aim of this prospective longitudinal study was to compare driving pressure and absolute PaO/FiO ratio in determining the best positive end-expiratory pressure (PEEP) level.
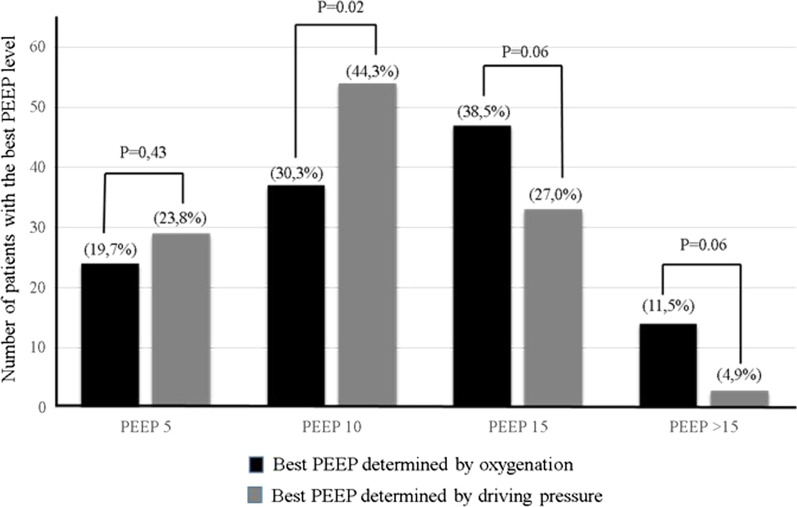
In 122 patients with acute respiratory distress syndrome, PEEP was increased until plateau pressure reached 30 cmHO at constant tidal volume, then decreased at 15-min intervals, to 15, 10, and 5 cmHO. The best PEEP by PaO/FiO ratio (PEEP) was defined as the highest PaO/FiO ratio obtained, and the best PEEP by driving pressure (PEEP) as the lowest driving pressure. The difference between the best PEEP levels was compared to a non-inferiority margin of 1.5 cmHO.
The best mean PEEP value was 11.9 ± 4.7 cmHO compared to 10.6 ± 4.1 cmHO for the best PEEP: mean difference = 1.3 cmHO (95% confidence interval [95% CI], 0.4-2.3; one-tailed P value, 0.36). Only 46 PEEP levels were the same with the two methods (37.7%; 95% CI 29.6-46.5). PEEP level was ≥ 15 cmHO in 61 (50%) patients with PEEP and 39 (32%) patients with PEEP (P = 0.001).
Depending on the method chosen, the best PEEP level varies. The best PEEP level is lower than the best PEEP level. Computing driving pressure is simple, faster and less invasive than measuring PaO. However, our results do not demonstrate that one method deserves preference over the other in terms of patient outcome.
#ACTRN12618000554268 . Registered 13 April 2018.
本前瞻性纵向研究旨在比较驱动压和绝对 PaO/FiO 比值在确定最佳呼气末正压(PEEP)水平方面的作用。
122 例急性呼吸窘迫综合征患者,在潮气量恒定的情况下,将 PEEP 增加至平台压达到 30cmH2O,然后每 15 分钟以 15、10 和 5cmH2O 的间隔降低 PEEP,直至达到最高 PaO/FiO 比值时的最佳 PEEP(PEEP),并定义为最佳 PEEP,以及达到最低驱动压时的最佳 PEEP(PEEP)。将最佳 PEEP 水平之间的差异与 1.5cmH2O 的非劣效性边界进行比较。
最佳平均 PEEP 值为 11.9±4.7cmH2O,最佳 PEEP:平均差值=1.3cmH2O(95%置信区间[95%CI],0.4-2.3;单侧 P 值,0.36)。两种方法相同的 PEEP 水平仅为 46 个(37.7%;95%CI 29.6-46.5)。PEEP 水平为≥15cmH2O 的患者中,PEEP 为 61 例(50%),PEEP 为 39 例(32%)(P=0.001)。
根据所选方法,最佳 PEEP 水平不同。最佳 PEEP 水平低于最佳 PEEP 水平。计算驱动压比测量 PaO 更简单、更快且侵入性更小。然而,我们的结果并未表明在患者预后方面,一种方法优于另一种方法。
#ACTRN12618000554268。于 2018 年 4 月 13 日注册。