Curtis Jeffrey R, Fox Kathleen M, Xie Fenglong, Su Yujie, Collier David, Clinton Cassie, Oko-Osi Hafiz
University of Alabama at Birmingham, Birmingham, AL, USA.
Amgen Inc., Thousand Oaks, CA, USA.
Rheumatol Ther. 2022 Oct;9(5):1329-1345. doi: 10.1007/s40744-022-00473-6. Epub 2022 Jul 14.
In patients with rheumatoid arthritis (RA), attaining remission or low disease activity (LDA), as recommended by the treat-to-target approach, has shown to yield improvement in symptoms and quality of life. However, limited evidence from real-world settings is available to support the premise that better disease control is associated with lower healthcare costs. This study fills in evidence gaps regarding the cost of care by RA disease activity (DA) states and by therapy.
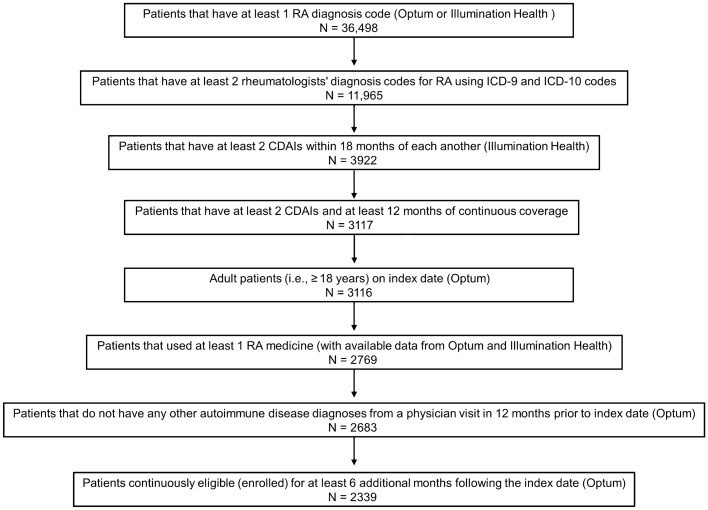
This retrospective cohort study linked medical and prescription claims from Optum Clinformatics Data Mart to electronic health record data from Illumination Health over 1/1/2010-3/31/2020. Mean annual costs for payers and patients were examined, stratifying on DA state and baseline use of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), biologics, and targeted synthetic (ts)DMARDs. Subgroup analysis examining within-person change in costs pre- and post-initiation of new therapy was also performed. Descriptive statistics, means, and boot-strapped confidence intervals were analyzed by DA state and by RA therapy. Furthermore, multivariate negative binomial regression analysis adjusting for key baseline characteristics was conducted.
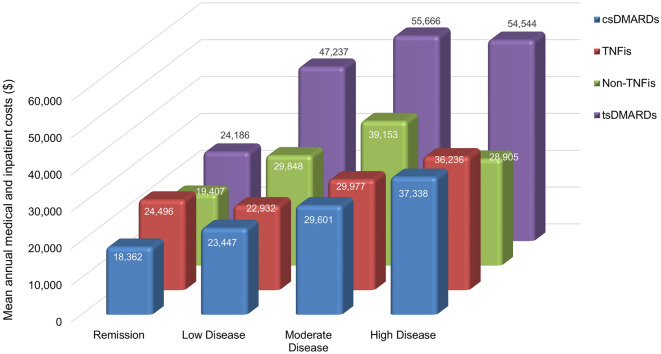
Of 2339 eligible patients, 19% were in remission, 40% in LDA, 29% in moderate DA (MDA), and 12% in high DA (HDA) at baseline. Mean annual costs during follow-up were substantially less for patients in remission ($40,072) versus those in MDA ($56,536) and HDA ($59,217). For patients in remission, csDMARD use was associated with the lowest mean annual cost ($25,575), tsDMARD was highest ($75,512), and tumor necrosis factor inhibitor (TNFi) ($69,846) and non-TNFi ($57,507) were intermediate. Among new TNFi (n = 137) and non-TNFi initiators (n = 107), 31% and 26% attained LDA/remission, respectively, and the time to achieve remission/LDA was numerically shorter in TNFi vs. non-TNFi initiators. For those on biologics, mean annual within-person medical and inpatient costs were lower after achieving LDA/remission, although pharmacy costs were higher.
Cost of care increased with increasing DA state, with patients in remission having the lowest costs. Optimizing DA has the potential for substantial savings in healthcare costs, although may be partially offset by the high cost of targeted RA therapies.
在类风湿性关节炎(RA)患者中,按照治疗目标方法的建议实现缓解或低疾病活动度(LDA),已显示出症状和生活质量得到改善。然而,来自现实世界环境的证据有限,无法支持更好的疾病控制与更低的医疗成本相关这一前提。本研究填补了关于RA疾病活动度(DA)状态和治疗方式的护理成本方面的证据空白。
这项回顾性队列研究将Optum临床信息数据集市的医疗和处方理赔数据与2010年1月1日至2020年3月31日期间Illumination Health的电子健康记录数据相链接。研究了支付方和患者的年均成本,按DA状态以及传统合成抗风湿药物(csDMARDs)、生物制剂和靶向合成(ts)DMARDs的基线使用情况进行分层。还进行了亚组分析,研究新疗法开始前后患者成本的个体内变化。通过DA状态和RA治疗方式分析描述性统计数据、均值和自助置信区间。此外,进行了调整关键基线特征的多变量负二项回归分析。
在2339名符合条件的患者中,基线时19%处于缓解状态,40%处于LDA,29%处于中度DA(MDA),12%处于高度DA(HDA)。随访期间,缓解状态患者的年均成本(40,072美元)显著低于MDA患者(56,536美元)和HDA患者(59,217美元)。对于缓解状态的患者,使用csDMARD的年均成本最低(25,575美元),tsDMARD最高(75,512美元),肿瘤坏死因子抑制剂(TNFi)(69,846美元)和非TNFi(57,507美元)处于中间水平。在新开始使用TNFi(n = 137)和非TNFi(n = 107)的患者中,分别有31%和26%达到LDA/缓解状态,且TNFi开始使用者达到缓解/LDA的时间在数值上比非TNFi开始使用者短。对于使用生物制剂的患者,达到LDA/缓解后个体内年均医疗和住院成本较低,尽管药房成本较高。
护理成本随着DA状态的增加而增加,缓解状态的患者成本最低。优化DA有可能大幅节省医疗成本,尽管可能会被靶向RA疗法的高成本部分抵消。