Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy.
Department of Rheumatology and Medical Sciences, ASST Pini-CTO, Milan, Italy.
Adv Ther. 2024 Sep;41(9):3706-3721. doi: 10.1007/s12325-024-02948-0. Epub 2024 Aug 7.
This study compared the clinical effectiveness of switching from tumor necrosis factor inhibitor (TNFi) to upadacitinib (TNFi-UPA), another TNFi (TNFi-TNFi), or an advanced therapy with another mechanism of action (TNFi-other MOA) in patients with rheumatoid arthritis (RA).
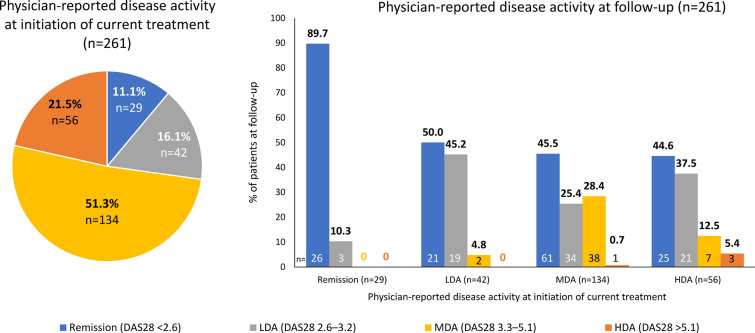
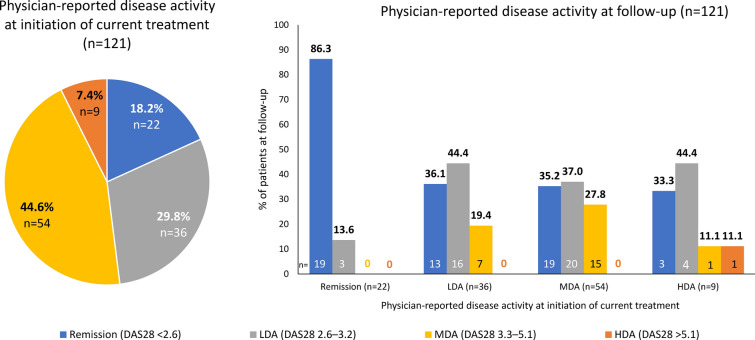
Data were drawn from the Adelphi RA Disease Specific Programme™, a cross-sectional survey administered to rheumatologists and their consulting patients in Germany, France, Italy, Spain, the UK, Japan, Canada, and the USA from May 2021 to January 2022. Patients who switched treatment from an initial TNFi were stratified by subsequent therapy of interest: TNFi-UPA, TNFi-TNFi, or TNFi-other MOA. Physician-reported clinical outcomes including disease activity (with formal DAS28 scoring available for 29% of patients) categorized as remission, low/moderate/high disease activity, as well as pain were recorded at initiation of current treatment and ≥ 6 months from treatment switch. Fatigue and treatment adherence were measured ≥ 6 months from treatment switch. Inverse-probability-weighted regression adjustment compared outcomes by subsequent class of therapy: TNFi-UPA versus TNFi-TNFi, or TNFi-UPA versus TNFi-other MOA.
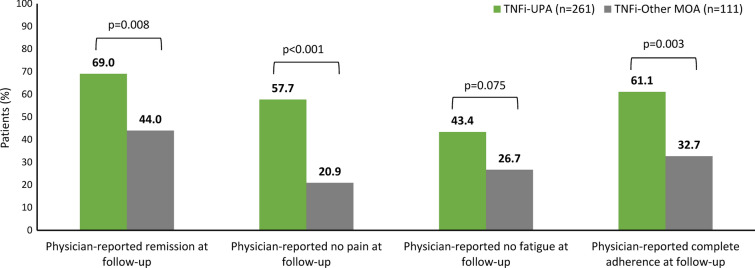
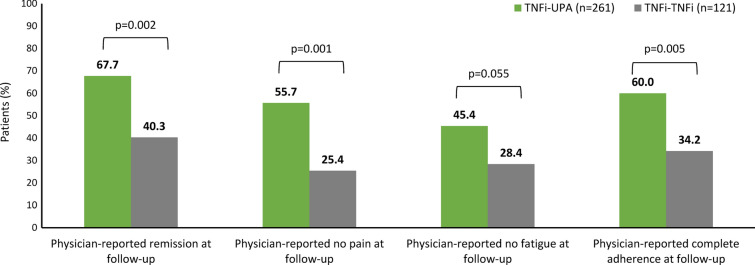
Of 503 patients who switched from their first TNFi, 261 were in TNFi-UPA, 128 in TNFi-TNFi, and 114 in TNFi-other MOA groups. At the time of switch, most patients had moderate/high disease activity (TNFi-UPA: 73%; TNFi-TNFi: 52%; TNFi-other MOA: 60%). After adjustment for differences in characteristics at point of switch, patients in TNFi-UPA group (n = 261) were significantly more likely to achieve physician-reported remission (67.7% vs. 40.3%; p = 0.0015), no pain (55.7% vs. 25.4%; p = 0.0007), and complete adherence (60.0% vs. 34.2%; p = 0.0049) compared with patients in TNFi-TNFi group (n = 121). Similar findings were observed for TNFi-UPA versus TNFi-other MOA groups (n = 111).
Patients who switched from TNFi to UPA had significantly better clinical outcomes of remission, no pain, and complete adherence than those who cycled TNFi or switched to another MOA.
本研究比较了在类风湿关节炎(RA)患者中,从肿瘤坏死因子抑制剂(TNFi)切换为乌帕替尼(TNFi-UPA)、另一种 TNFi(TNFi-TNFi)或另一种作用机制的先进治疗方法(TNFi-其他 MOA)的临床效果。
数据来自 Adelphi RA 疾病专项计划™,这是一项在 2021 年 5 月至 2022 年 1 月期间,从德国、法国、意大利、西班牙、英国、日本、加拿大和美国的风湿病医生及其就诊患者中进行的横断面调查。根据后续治疗的不同,将接受初始 TNFi 治疗的患者分为以下亚组:TNFi-UPA、TNFi-TNFi 或 TNFi-其他 MOA。在开始当前治疗时和治疗转换后≥6 个月时,记录了医生报告的临床结果,包括疾病活动度(对于 29%的患者可进行正式 DAS28 评分),分为缓解、低/中/高度疾病活动度,以及疼痛。在治疗转换后≥6 个月时,测量了疲劳和治疗依从性。通过逆概率加权回归调整比较了后续治疗类别的结果:TNFi-UPA 与 TNFi-TNFi,或 TNFi-UPA 与 TNFi-其他 MOA。
在 503 名从其首种 TNFi 治疗中转换的患者中,261 名患者进入 TNFi-UPA 组,128 名患者进入 TNFi-TNFi 组,114 名患者进入 TNFi-其他 MOA 组。在转换时,大多数患者的疾病活动度为中/高度(TNFi-UPA:73%;TNFi-TNFi:52%;TNFi-其他 MOA:60%)。在调整了转换时的特征差异后,与 TNFi-TNFi 组(n=121)相比,TNFi-UPA 组(n=261)的患者更有可能达到医生报告的缓解(67.7%比 40.3%;p=0.0015)、无疼痛(55.7%比 25.4%;p=0.0007)和完全依从(60.0%比 34.2%;p=0.0049)。TNFi-UPA 与 TNFi-其他 MOA 组(n=111)也观察到类似的发现。
与循环 TNFi 或切换到另一种 MOA 的患者相比,从 TNFi 切换到 UPA 的患者的缓解、无疼痛和完全依从的临床结局显著更好。