Institute of Reproductive and Developmental Biology (IRDB), Department of Metabolism, Digestion and Reproduction-Surgery and Cancer, Faculty of Medicine, Imperial College London, London, UK; Imperial College Healthcare NHS Trust, London, UK.
Institute of Reproductive and Developmental Biology (IRDB), Department of Metabolism, Digestion and Reproduction-Surgery and Cancer, Faculty of Medicine, Imperial College London, London, UK; Knowledge Translation Program, Li Ka Shing Knowledge Institute, St Michael's Hospital, Toronto, ON, Canada; Institute for Health Policy, Management and Evaluation, University of Toronto, Toronto, ON, Canada.
Lancet Oncol. 2022 Aug;23(8):1097-1108. doi: 10.1016/S1470-2045(22)00334-5. Epub 2022 Jul 11.
The trade-off between comparative effectiveness and reproductive morbidity of different treatment methods for cervical intraepithelial neoplasia (CIN) remains unclear. We aimed to determine the risks of treatment failure and preterm birth associated with various treatment techniques.
In this systematic review and network meta-analysis, we searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials database for randomised and non-randomised studies reporting on oncological or reproductive outcomes after CIN treatments from database inception until March 9, 2022, without language restrictions. We included studies of women with CIN, glandular intraepithelial neoplasia, or stage IA1 cervical cancer treated with excision (cold knife conisation [CKC], laser conisation, and large loop excision of the transformation zone [LLETZ]) or ablation (radical diathermy, laser ablation, cold coagulation, and cryotherapy). We excluded women treated with hysterectomy. The primary outcomes were any treatment failure (defined as any abnormal histology or cytology) and preterm birth (<37 weeks of gestation). The network for preterm birth also included women with untreated CIN (untreated colposcopy group). The main reference group was LLETZ for treatment failure and the untreated colposcopy group for preterm birth. For randomised controlled trials, we extracted group-level summary data, and for observational studies, we extracted relative treatment effect estimates adjusted for potential confounders, when available, and we did random-effects network meta-analyses to obtain odds ratios (ORs) with 95% CIs. We assessed within-study and across-study risk of bias using Cochrane tools. This systematic review is registered with PROSPERO, CRD42018115495 and CRD42018115508.
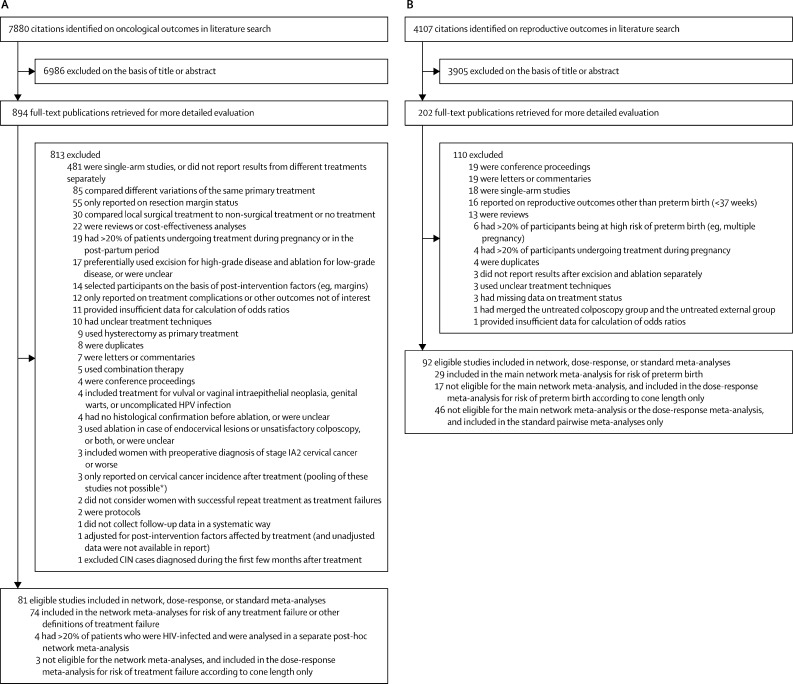
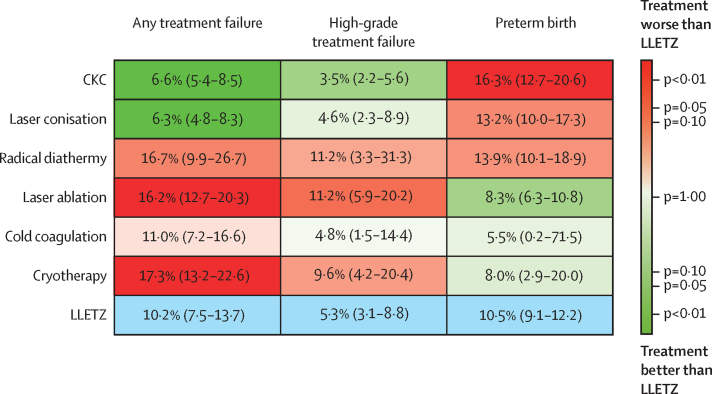
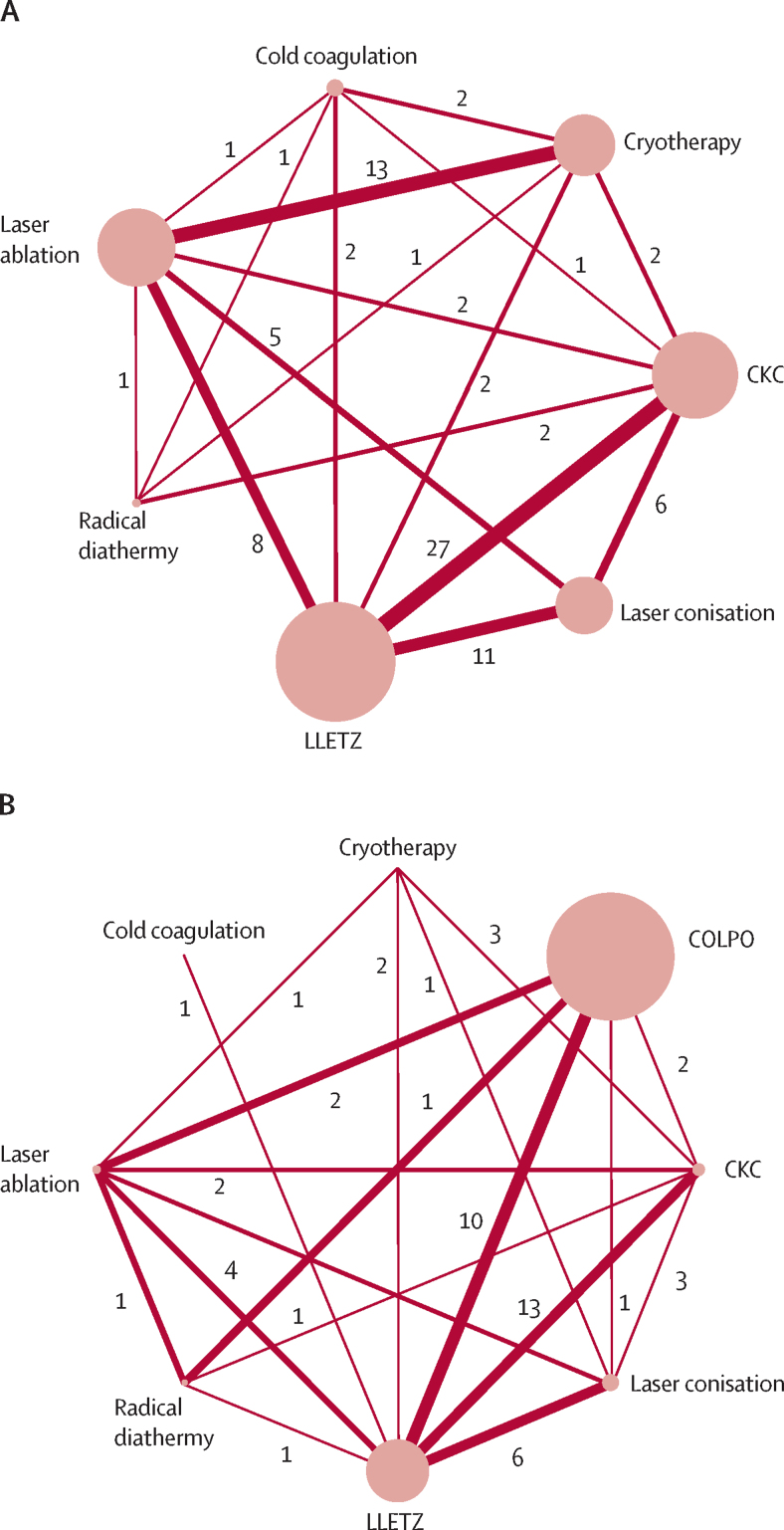
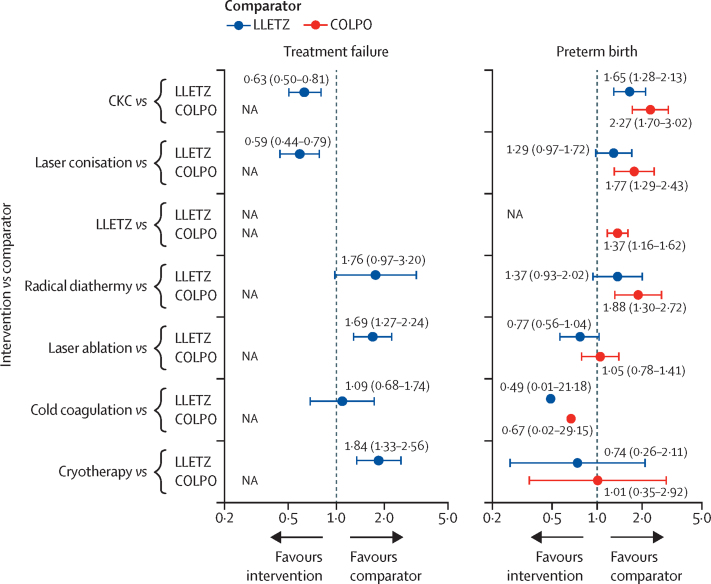
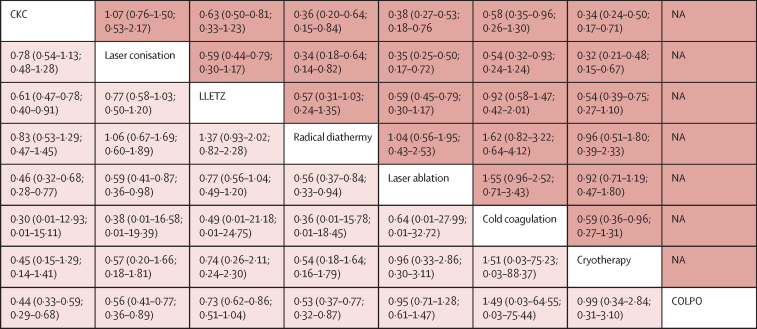
7880 potential citations were identified for the outcome of treatment failure and 4107 for the outcome of preterm birth. After screening and removal of duplicates, the network for treatment failure included 19 240 participants across 71 studies (25 randomised) and the network for preterm birth included 68 817 participants across 29 studies (two randomised). Compared with LLETZ, risk of treatment failure was reduced for other excisional methods (laser conisation: OR 0·59 [95% CI 0·44-0·79] and CKC: 0·63 [0·50-0·81]) and increased for laser ablation (1·69 [1·27-2·24]) and cryotherapy (1·84 [1·33-2·56]). No differences were found for the comparison of cold coagulation versus LLETZ (1·09 [0·68-1·74]) but direct data were based on two small studies only. Compared with the untreated colposcopy group, risk of preterm birth was increased for all excisional techniques (CKC: 2·27 [1·70-3·02]; laser conisation: 1·77 [1·29-2·43]; and LLETZ: 1·37 [1·16-1·62]), whereas no differences were found for ablative methods (laser ablation: 1·05 [0·78-1·41]; cryotherapy: 1·01 [0·35-2·92]; and cold coagulation: 0·67 [0·02-29·15]). The evidence was based mostly on observational studies with their inherent risks of bias, and the credibility of many comparisons was low.
More radical excisional techniques reduce the risk of treatment failure but increase the risk of subsequent preterm birth. Although there is uncertainty, ablative treatments probably do not increase risk of preterm birth, but are associated with higher failure rates than excisional techniques. Although we found LLETZ to have balanced effectiveness and reproductive morbidity, treatment choice should rely on a woman's age, size and location of lesion, and future family planning.
National Institute for Health and Care Research: Research for Patient Benefit.
不同治疗方法治疗宫颈上皮内瘤变(CIN)的有效性和生殖发病率之间的权衡仍不清楚。我们旨在确定与各种治疗技术相关的治疗失败和早产风险。
在这项系统评价和网络荟萃分析中,我们检索了 MEDLINE、Embase 和 Cochrane 对照试验中心注册库,以查找自数据库成立至 2022 年 3 月 9 日为止,报告 CIN 治疗后肿瘤学或生殖结局的随机和非随机研究,无语言限制。我们纳入了 CIN、腺上皮内瘤变或 IA1 期宫颈癌的女性接受切除术(冷刀锥切术[CKC]、激光锥切术和转化区大环形切除术[LLETZ])或消融术(根治性热疗、激光消融术、冷凝固术和冷冻疗法)治疗的研究。我们排除了接受子宫切除术治疗的女性。主要结局是任何治疗失败(定义为任何异常组织学或细胞学)和早产(<37 周妊娠)。早产网络还包括未经治疗的 CIN 女性(未经治疗的阴道镜检查组)。主要参考组为 LLETZ 治疗失败和未经治疗的阴道镜检查组的早产。对于随机对照试验,我们提取了组水平汇总数据,对于观察性研究,我们提取了在可用时经潜在混杂因素调整的相对治疗效果估计值,并进行了随机效应网络荟萃分析,以获得比值比(OR)及其 95%置信区间(CI)。我们使用 Cochrane 工具评估了研究内和研究间的偏倚风险。本系统评价已在 PROSPERO、CRD42018115495 和 CRD42018115508 上注册。
针对治疗失败的结局,共识别出 7880 条潜在的引用,针对早产的结局,共识别出 4107 条引用。在筛选并去除重复项后,治疗失败网络纳入了 71 项研究(25 项随机研究)的 19240 名参与者,早产网络纳入了 29 项研究(2 项随机研究)的 68817 名参与者。与 LLETZ 相比,其他切除术方法(激光锥切术:OR 0.59 [95%CI 0.44-0.79]和 CKC:0.63 [0.50-0.81])降低了治疗失败的风险,而激光消融术(1.69 [1.27-2.24])和冷冻疗法(1.84 [1.33-2.56])则增加了治疗失败的风险。冷凝固术与 LLETZ 相比,差异无统计学意义(1.09 [0.68-1.74]),但直接数据仅基于两项小型研究。与未经治疗的阴道镜检查组相比,所有切除术技术(CKC:2.27 [1.70-3.02];激光锥切术:1.77 [1.29-2.43];和 LLETZ:1.37 [1.16-1.62])增加了早产的风险,而消融方法则无差异(激光消融术:1.05 [0.78-1.41];冷冻疗法:1.01 [0.35-2.92];和冷凝固术:0.67 [0.02-29.15])。证据主要基于观察性研究,存在固有偏倚风险,许多比较的可信度较低。
更激进的切除术技术降低了治疗失败的风险,但增加了随后早产的风险。虽然存在不确定性,但消融治疗可能不会增加早产的风险,但与切除术技术相比,其失败率更高。虽然我们发现 LLETZ 具有平衡的有效性和生殖发病率,但治疗选择应取决于女性的年龄、病变的大小和位置以及未来的家庭计划。
英国国家卫生与保健研究院:研究造福患者。