Department of Medical Oncology, Fujian Medical University Cancer Hospital and Fujian Cancer Hospital, Fuzhou, China.
Cancer Bio-immunotherapy Center, Fujian Medical University Cancer Hospital and Fujian Cancer Hospital, Fuzhou, China.
Front Immunol. 2022 Jul 1;13:725679. doi: 10.3389/fimmu.2022.725679. eCollection 2022.
Although melanoma is generally regarded as an immunogenic cancer that will respond to immune checkpoint inhibitors (ICIs), melanomas with amplification respond poorly to these therapies. Further understanding how amplification impacts the effectiveness of ICI therapy is important for the design of future clinical trials.
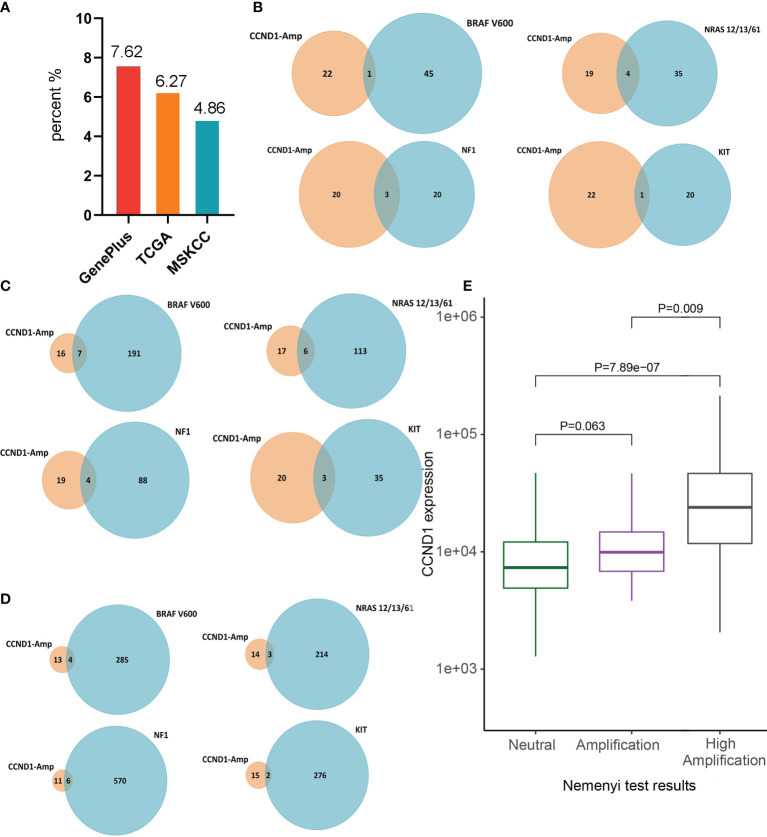
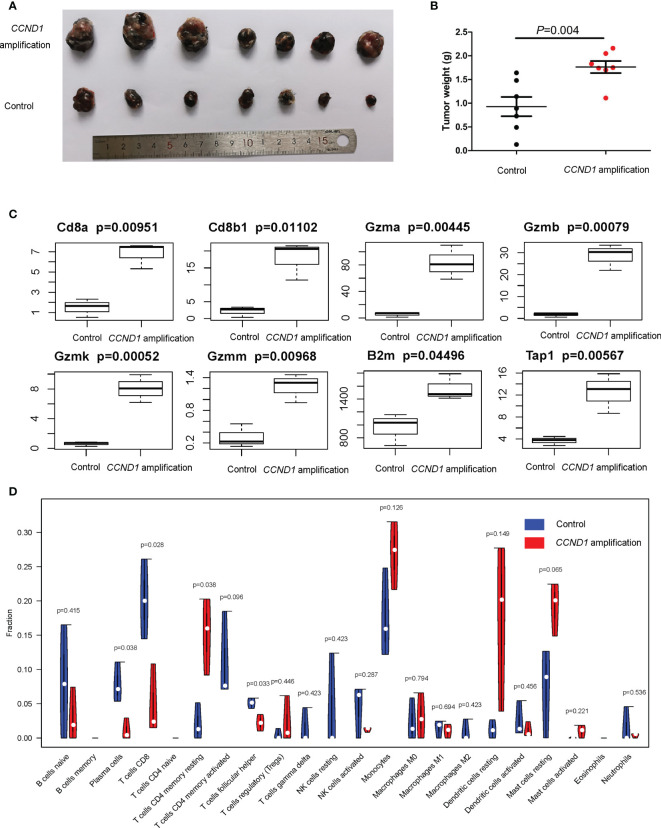
We used data from tumor samples taken from Chinese patients with melanoma analyzed at the Geneplus Institute (=302), as well as data from the Cancer Genome Atlas (TCGA) database (=367) and the Memorial Sloan Kettering Cancer Center (MSKCC) database (=350) to estimate the prevalence of amplification in melanoma, interrogate the relationship between amplification and survival in patients with melanoma, and explore the molecular mechanisms of amplification. We also established a murine model of melanoma harboring amplification and utilized RNA-seq to verify the findings from human tissue samples.
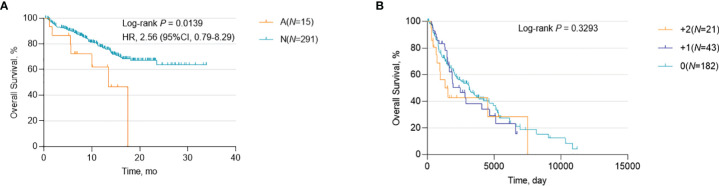
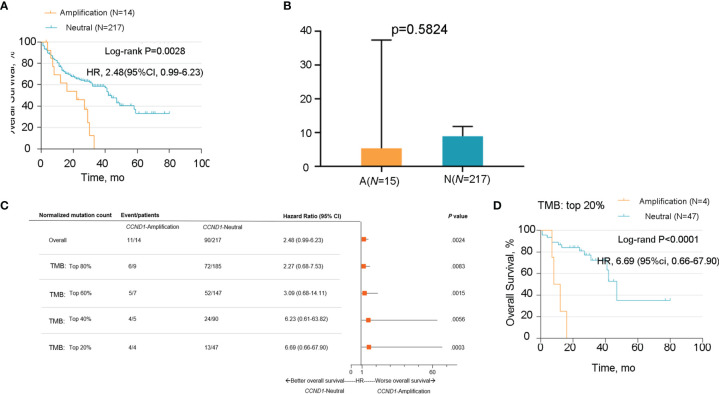
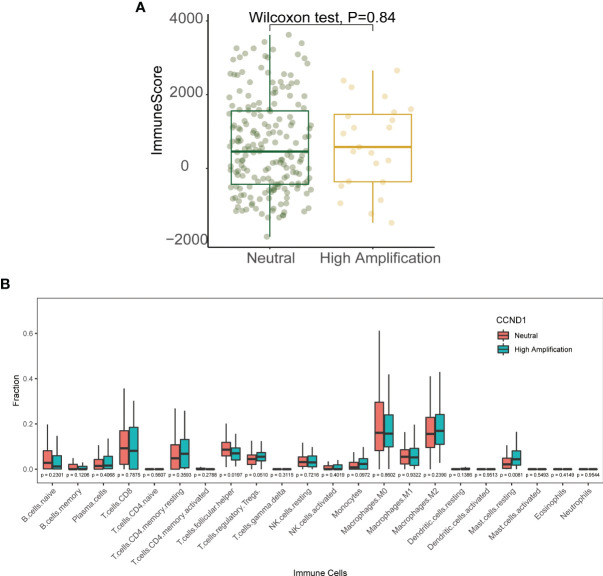
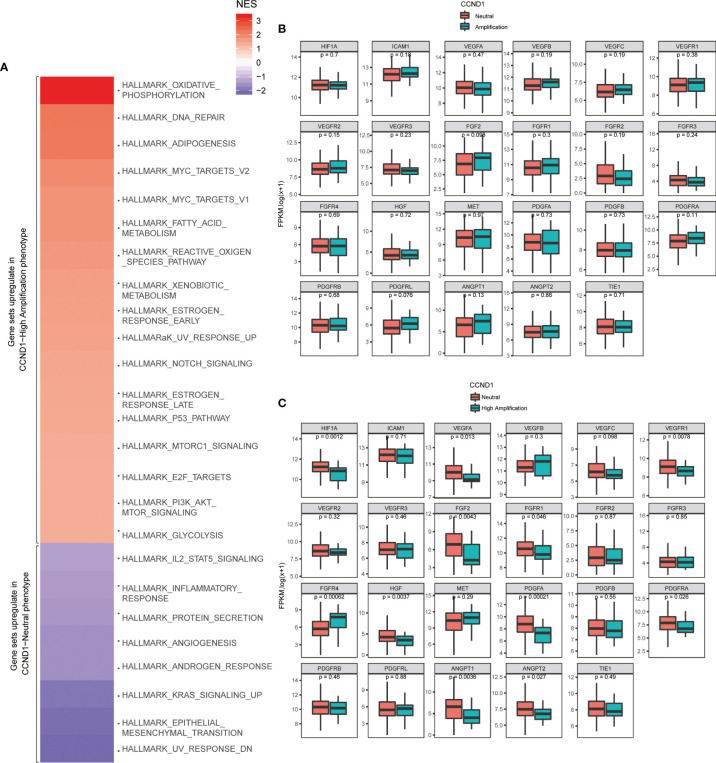
Data from all three sources revealed a low frequency of amplification co-occurring with , , , and mutations. Data from TCGA did not show a statistically significant correlation between amplification and prognosis, irrespective of ICI use. In contrast, the MSKCC cohort showed that amplification was an unfavorable prognostic factor for patients with melanoma, especially for patients who received ICIs and had a high tumor mutation burden (TMB). The TCGA data showed that amplification was associated with a higher proportion of immunosuppressive cells (Treg cells and M2 macrophages) and a lower proportion of immune boosting cells (follicular helper T cells naïve B cells, CD8 T cells). Murine models supported the association between a suppressive immune microenvironment and amplification; tumors with amplification had reduced mRNA expression of CD8, Gzm, B2m and Tap1, significantly higher proportions of resting CD4 memory T cells and significantly lower proportions of plasma cells, CD8 T cells, and T follicular helper cells. Furthermore, a Gene Set Enrichment Analysis (GSEA) analysis of data from the TCGA database suggested that signaling pathways involved in oxidative phosphorylation, reactive oxygen species, adipogenesis, fatty acid metabolism, DNA repair, and Myc targets were differentially enriched in melanoma tumors with amplification. Finally, we observed a notable reduction in levels of angiogenesis-related molecules (encoded by , , , , and ) in a high amplification group from the TCGA database.
Melanoma with amplification is an independent genomic subtype associated with a poor prognosis, an immunosuppressive TME, activated oxidative and lipid metabolism, and down-regulated angiogenesis. Therefore, avoiding ICIs and antiangiogenic agents, while employing CDK4/6 inhibitors alone or in combination with ICIs, and targeting oxidative and lipid metabolism pathways, may be effective therapeutic strategies for melanoma patients harboring amplification.
尽管黑色素瘤通常被认为是一种对免疫检查点抑制剂(ICIs)有反应的免疫原性癌症,但存在 扩增的黑色素瘤对这些治疗反应不佳。进一步了解 扩增如何影响 ICI 治疗的效果对于未来临床试验的设计很重要。
我们使用了来自中国黑色素瘤患者肿瘤样本的数据,这些样本是在 Geneplus 研究所(=302)进行分析的,以及来自癌症基因组图谱(TCGA)数据库(=367)和纪念斯隆凯特琳癌症中心(MSKCC)数据库(=350)的数据,以估计黑色素瘤中 扩增的流行率,探究 扩增与黑色素瘤患者生存之间的关系,并探索 扩增的分子机制。我们还建立了携带 扩增的黑色素瘤小鼠模型,并利用 RNA-seq 来验证来自人类组织样本的发现。
来自这三个来源的数据都显示出 扩增与 、 、 和 突变同时发生的频率较低。TCGA 数据未显示 扩增与预后之间存在统计学显著相关性,无论是否使用 ICI 治疗均如此。相比之下,MSKCC 队列显示, 扩增是黑色素瘤患者的不利预后因素,尤其是对接受 ICI 治疗且肿瘤突变负担较高的患者。TCGA 数据显示, 扩增与较高比例的免疫抑制细胞(调节性 T 细胞和 M2 巨噬细胞)和较低比例的免疫增强细胞(滤泡辅助 T 细胞幼稚 B 细胞、CD8 T 细胞)相关。小鼠模型支持抑制性免疫微环境与 扩增之间的关联;携带 扩增的肿瘤 CD8、Gzm、B2m 和 Tap1 的 mRNA 表达水平降低,静止 CD4 记忆 T 细胞的比例显著升高,浆细胞、CD8 T 细胞和滤泡辅助 T 细胞的比例显著降低。此外,对 TCGA 数据库中数据进行基因集富集分析(GSEA)分析表明,黑色素瘤肿瘤中涉及氧化磷酸化、活性氧、脂肪生成、脂肪酸代谢、DNA 修复和 Myc 靶点的信号通路在 扩增的黑色素瘤肿瘤中存在差异富集。最后,我们在 TCGA 数据库的高 扩增组中观察到血管生成相关分子(由 、 、 、 和 编码)的水平显著降低。
携带 扩增的黑色素瘤是一种独立的基因组亚型,与不良预后、免疫抑制性 TME、激活的氧化和脂质代谢以及下调的血管生成相关。因此,避免使用 ICI 和抗血管生成药物,而单独使用 CDK4/6 抑制剂或与 ICI 联合使用,并针对氧化和脂质代谢途径进行靶向治疗,可能是携带 扩增的黑色素瘤患者的有效治疗策略。