Pallauf Maximilian, König Frederik, D'Andrea David, Laukhtina Ekaterina, Mostafaei Hadi, Motlagh Reza Sari, Quhal Fahad, Aydh Abdulmajeed, Yanagisawa Takafumi, Kawada Tatsushi, Rajwa Pawel, Lusuardi Lukas, Soria Francesco, Karakiewicz Pierre I, Rouprêt Morgan, Rink Michael, Lotan Yair, Margulis Vitaly, Singla Nirmish, Xylinas Evanguelos, Shariat Shahrokh F, Pradere Benjamin
Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Department of Urology, University Hospital Salzburg, Paracelsus Medical University, Salzburg, Austria.
Front Oncol. 2022 Jul 1;12:907975. doi: 10.3389/fonc.2022.907975. eCollection 2022.
Current guidelines recommend assessing the prognosis in high-risk upper tract urothelial carcinoma patients (UTUC) after surgery. However, no specific method is endorsed. Among the various prognostic models, nomograms represent an easy and accurate tool to predict the individual probability for a specific event. Therefore, identifying the best-suited nomogram for each setting seems of great interest to the patient and provider.
To identify, summarize and compare postoperative UTUC nomograms predicting oncologic outcomes. To estimate the overall performance of the nomograms and identify the most reliable predictors. To create a reference tool for postoperative UTUC nomograms, physicians can use in clinical practice.
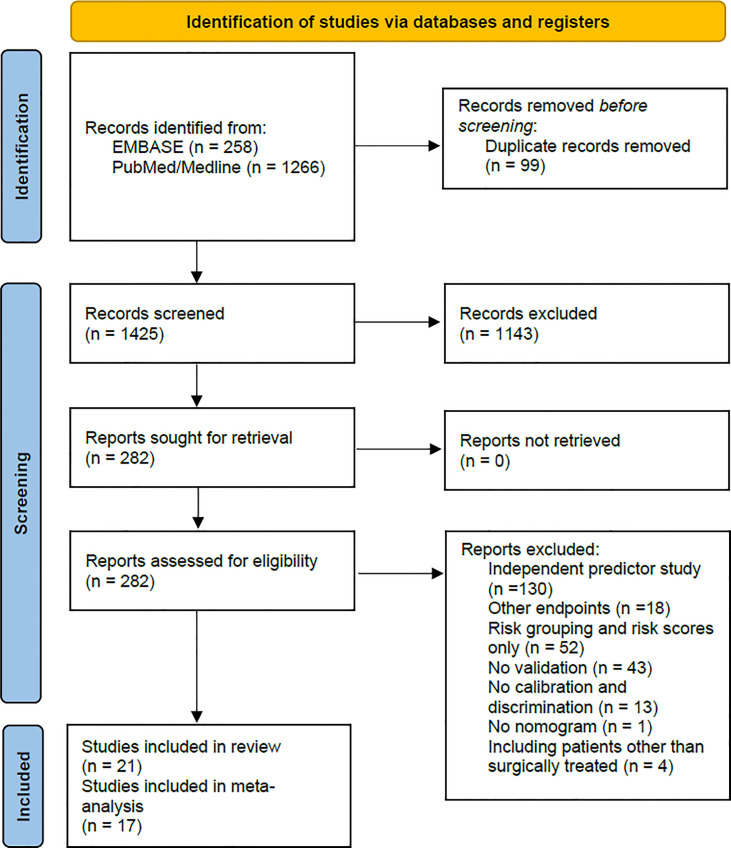
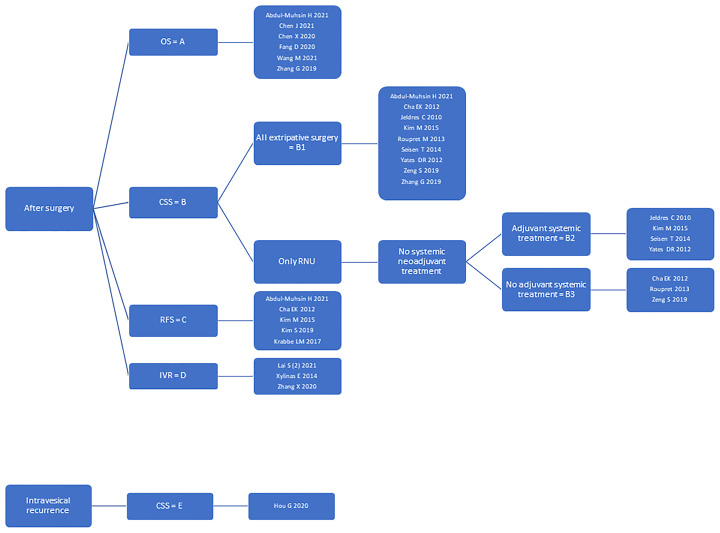
A systematic review was conducted following the recommendations of Cochrane's Prognosis Methods Group. Medline and EMBASE databases were searched for studies published before December 2021. Nomograms were grouped according to outcome measurements, the purpose of use, and inclusion and exclusion criteria. Random-effects meta-analyses were performed to estimate nomogram group performance and predictor reliability. Reference tables summarizing the nomograms' important characteristics were created.
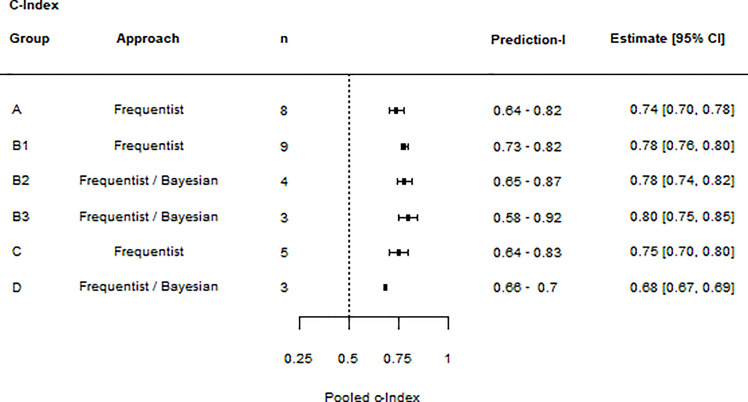
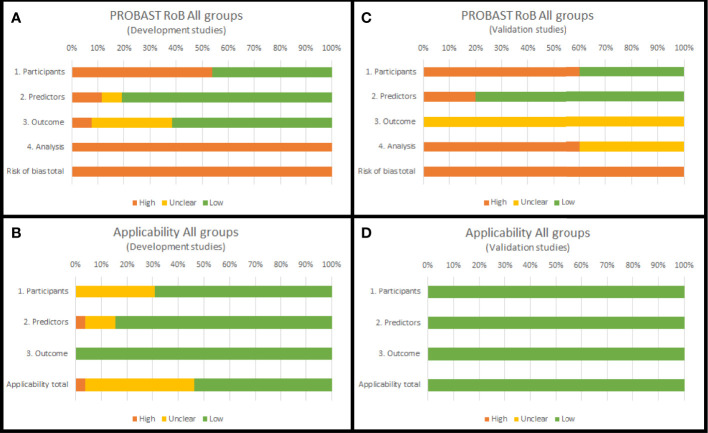
The systematic review identified 26 nomograms. Only four were externally validated. Study heterogeneity was significant, and the overall Risk of Bias (RoB) was high. Nomogram groups predicting overall survival (OS), recurrence-free survival (RFS), and intravesical recurrence (IVR) had moderate discrimination accuracy (c-Index summary estimate with 95% confidence interval [95% CI] and prediction interval [PI] > 0.6). Nomogram groups predicting cancer-specific survival (CSS) had good discrimination accuracy (c-Index summary estimate with 95% CI and PI > 0.7). Advanced pathological tumor stage (≥ pT3) was the most reliable predictor of OS. Pathological tumor stage (≥ pT2), age, and lymphovascular invasion (LVI) were the most reliable predictors of CSS. LVI was the most reliable predictor of RFS.
Despite a moderate to good discrimination accuracy, severe heterogeneity discourages the uninformed use of postoperative prognostic UTUC nomograms. For nomograms to become of value in a generalizable population, future research must invest in external validation and assessment of clinical utility. Meanwhile, this systematic review serves as a reference tool for physicians choosing nomograms based on individual needs.
https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=282596, identifier PROSPERO [CRD42021282596].
当前指南建议对高危上尿路尿路上皮癌(UTUC)患者术后的预后进行评估。然而,尚无得到认可的具体方法。在各种预后模型中,列线图是预测特定事件个体概率的一种简便且准确的工具。因此,为每种情况确定最适合的列线图似乎对患者和医疗服务提供者都非常有意义。
识别、总结和比较预测肿瘤学结局的UTUC术后列线图。评估列线图的整体性能并确定最可靠的预测因素。创建一个UTUC术后列线图的参考工具,供医生在临床实践中使用。
按照Cochrane预后方法组的建议进行系统评价。检索了Medline和EMBASE数据库中2021年12月之前发表的研究。根据结局测量、使用目的以及纳入和排除标准对列线图进行分组。进行随机效应荟萃分析以评估列线图组的性能和预测因素的可靠性。创建了总结列线图重要特征的参考表。
系统评价共识别出26个列线图。只有4个经过外部验证。研究异质性显著,总体偏倚风险较高。预测总生存期(OS)、无复发生存期(RFS)和膀胱内复发(IVR)的列线图组具有中等的区分准确性(c指数汇总估计值及其95%置信区间[95%CI]和预测区间[PI]>0.6)。预测癌症特异性生存期(CSS)的列线图组具有良好的区分准确性(c指数汇总估计值及其95%CI和PI>0.7)。高级别病理肿瘤分期(≥pT3)是OS最可靠的预测因素。病理肿瘤分期(≥pT2)、年龄和淋巴管侵犯(LVI)是CSS最可靠的预测因素。LVI是RFS最可靠的预测因素。
尽管区分准确性中等至良好,但严重的异质性不鼓励盲目使用UTUC术后预后列线图。为了使列线图在可推广的人群中具有价值,未来的研究必须投入到外部验证和临床效用评估中。同时,本系统评价可作为医生根据个体需求选择列线图的参考工具。
https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=282596,标识符PROSPERO [CRD42021282596] 。