Ratcliffe Helen, Tiley K S, Andrews Nick, Amirthalingam Gayatri, Vichos I, Morey E, Douglas N L, Marinou S, Plested Emma, Aley Parvinder, Galiza Eva P, Faust Saul N, Hughes S, Murray Clare S, Roderick Marion, Shackley Fiona, Oddie Sam J, Lees Tim, Turner D P J, Raman M, Owens Stephen, Turner Paul, Cockerill H, Lopez Bernal J, Linley E, Borrow Ray, Brown Kevin, Ramsay Mary Elizabeth, Voysey M, Snape Matthew D
Department of Paediatrics, University of Oxford, Oxford, UK
Department of Paediatrics, University of Oxford, Oxford, UK.
Arch Dis Child. 2023 Jan 19;108(2):123-130. doi: 10.1136/archdischild-2022-324375.
To understand community seroprevalence of SARS-CoV-2 in children and adolescents. This is vital to understanding the susceptibility of this cohort to COVID-19 and to inform public health policy for disease control such as immunisation.
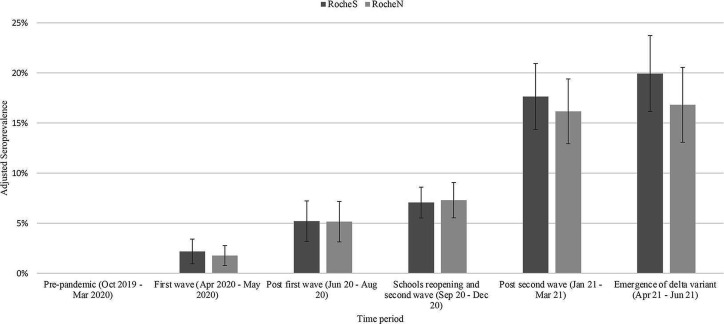
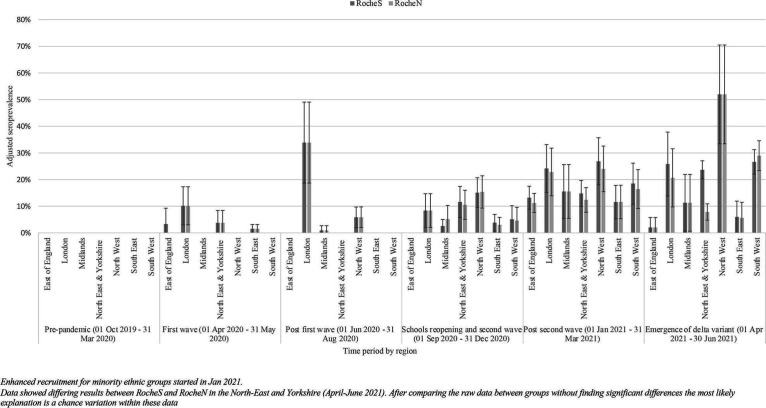
We conducted a community-based cross-sectional seroprevalence study in participants aged 0-18 years old recruiting from seven regions in England between October 2019 and June 2021 and collecting extensive demographic and symptom data. Serum samples were tested for antibodies against SARS-CoV-2 spike and nucleocapsid proteins using Roche assays processed at UK Health Security Agency laboratories. Prevalence estimates were calculated for six time periods and were standardised by age group, ethnicity and National Health Service region.
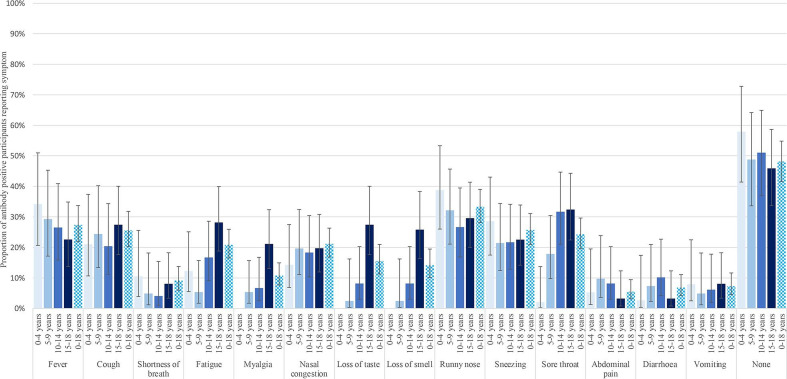
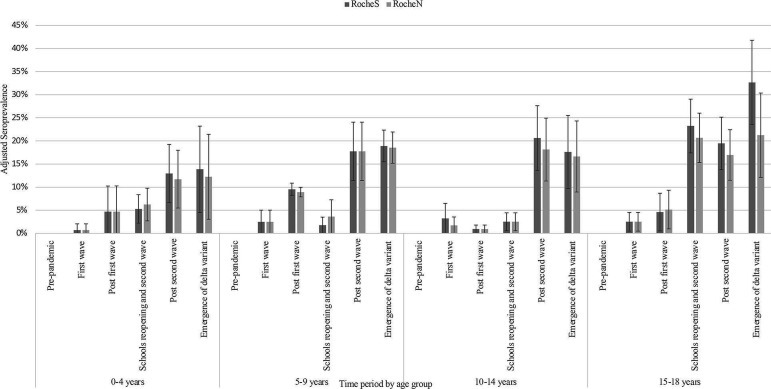
Post-first wave (June-August 2020), the (anti-spike IgG) adjusted seroprevalence was 5.2%, varying from 0.9% (participants 10-14 years old) to 9.5% (participants 5-9 years old). By April-June 2021, this had increased to 19.9%, varying from 13.9% (participants 0-4 years old) to 32.7% (participants 15-18 years old). Minority ethnic groups had higher risk of SARS-CoV-2 seropositivity than white participants (OR 1.4, 95% CI 1.0 to 2.0), after adjusting for sex, age, region, time period, deprivation and urban/rural geography. In children <10 years, there were no symptoms or symptom clusters that reliably predicted seropositivity. Overall, 48% of seropositive participants with complete questionnaire data recalled no symptoms between February 2020 and their study visit.
Approximately one-third of participants aged 15-18 years old had evidence of antibodies against SARS-CoV-2 prior to the introduction of widespread vaccination. These data demonstrate that ethnic background is independently associated with risk of SARS-CoV-2 infection in children.
NCT04061382.
了解儿童和青少年中新冠病毒(SARS-CoV-2)的社区血清阳性率。这对于了解该人群对新冠病毒病(COVID-19)的易感性以及为疾病控制(如免疫接种)的公共卫生政策提供信息至关重要。
我们在2019年10月至2021年6月期间,对来自英格兰七个地区的0至18岁参与者进行了一项基于社区的横断面血清阳性率研究,并收集了广泛的人口统计学和症状数据。使用在英国卫生安全局实验室处理的罗氏检测法,对血清样本进行针对SARS-CoV-2刺突蛋白和核衣壳蛋白的抗体检测。计算了六个时间段的患病率估计值,并按年龄组、种族和国民保健服务地区进行了标准化。
在第一波疫情之后(2020年6月至8月),调整后的(抗刺突IgG)血清阳性率为5.2%,从0.9%(10至14岁参与者)到9.5%(5至9岁参与者)不等。到2021年4月至6月,这一比例增至19.9%,从13.9%(0至4岁参与者)到32.7%(15至18岁参与者)不等。在调整了性别、年龄、地区、时间段、贫困程度和城乡地理因素后,少数族裔群体的SARS-CoV-2血清阳性风险高于白人参与者(比值比1.4,95%置信区间1.0至2.0)。在10岁以下儿童中,没有可靠地预测血清阳性的症状或症状群。总体而言,在有完整问卷数据的血清阳性参与者中,48%回忆起在2020年2月至其研究访视期间没有症状。
在广泛接种疫苗之前,约三分之一的15至18岁参与者有针对SARS-CoV-2的抗体证据。这些数据表明,种族背景与儿童SARS-CoV-2感染风险独立相关。
NCT04061382。