Lowe Center for Thoracic Oncology, Dana-Farber Cancer Institute, Boston, USA.
Thoracic Oncology Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, USA.
Ann Oncol. 2022 Oct;33(10):1029-1040. doi: 10.1016/j.annonc.2022.07.005. Epub 2022 Jul 22.
Allele-specific KRAS inhibitors are an emerging class of cancer therapies. KRAS-mutant (KRAS) non-small-cell lung cancers (NSCLCs) exhibit heterogeneous outcomes, driven by differences in underlying biology shaped by co-mutations. In contrast to KRAS NSCLC, KRAS NSCLC is associated with low/never-smoking status and is largely uncharacterized.
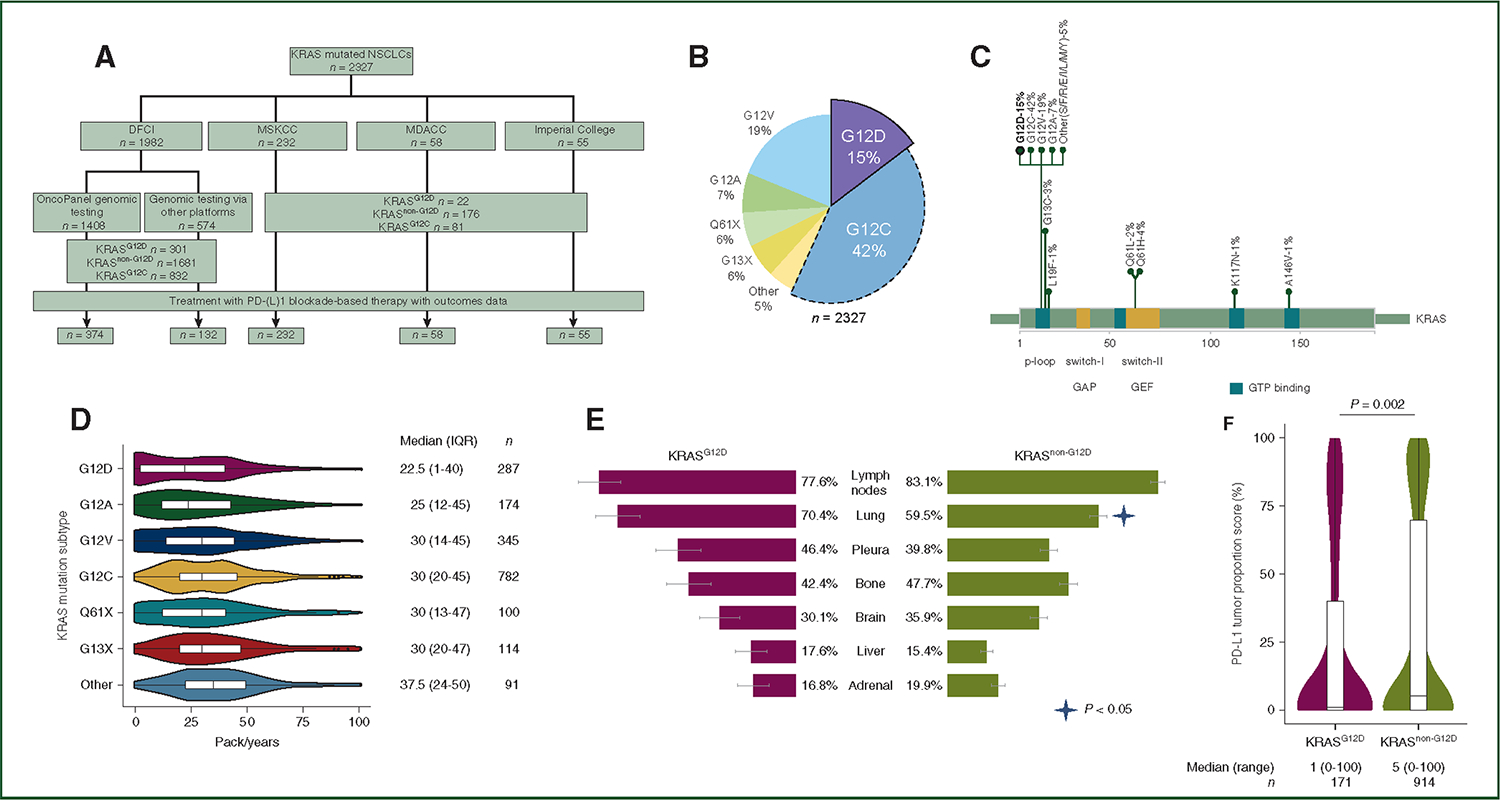
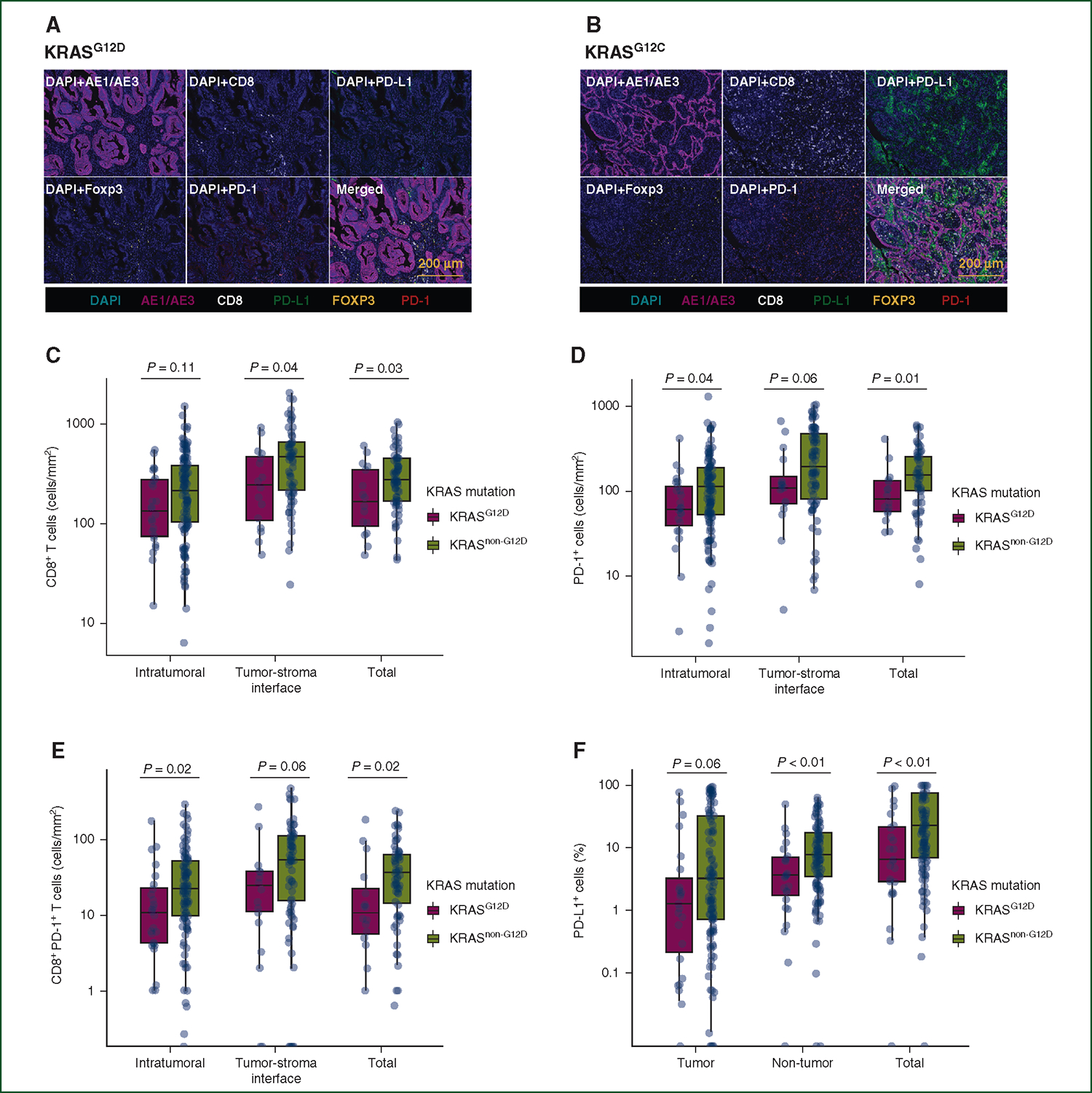
Clinicopathologic and genomic information were collected from patients with NSCLCs harboring a KRAS mutation at the Dana-Farber Cancer Institute (DFCI), Memorial Sloan Kettering Cancer Center, MD Anderson Cancer Center, and Imperial College of London. Multiplexed immunofluorescence for CK7, programmed cell death protein 1 (PD-1), programmed death-ligand 1 (PD-L1), Foxp3, and CD8 was carried out on a subset of samples with available tissue at the DFCI. Clinical outcomes to PD-(L)1 inhibition ± chemotherapy were analyzed according to KRAS mutation subtype.
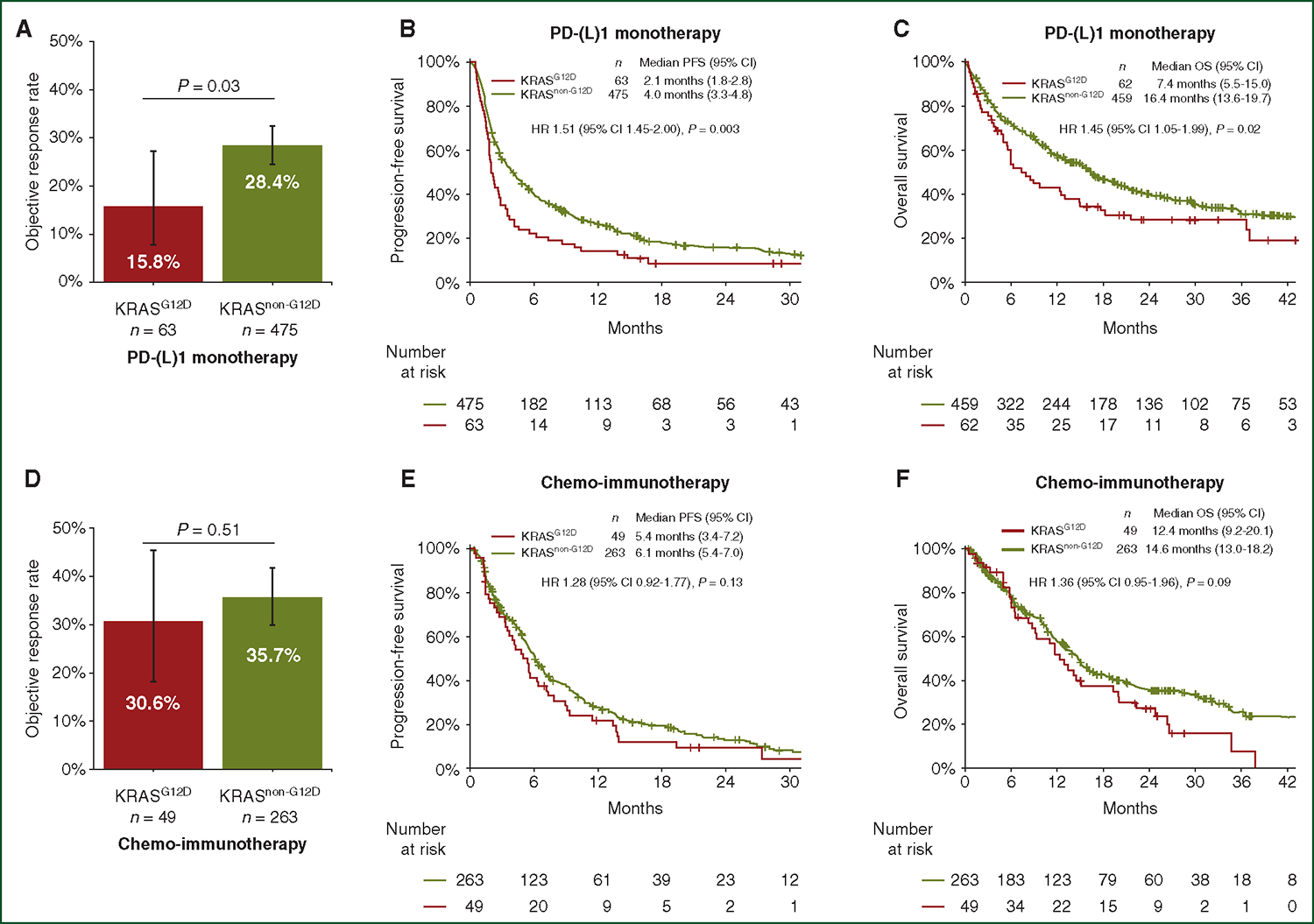
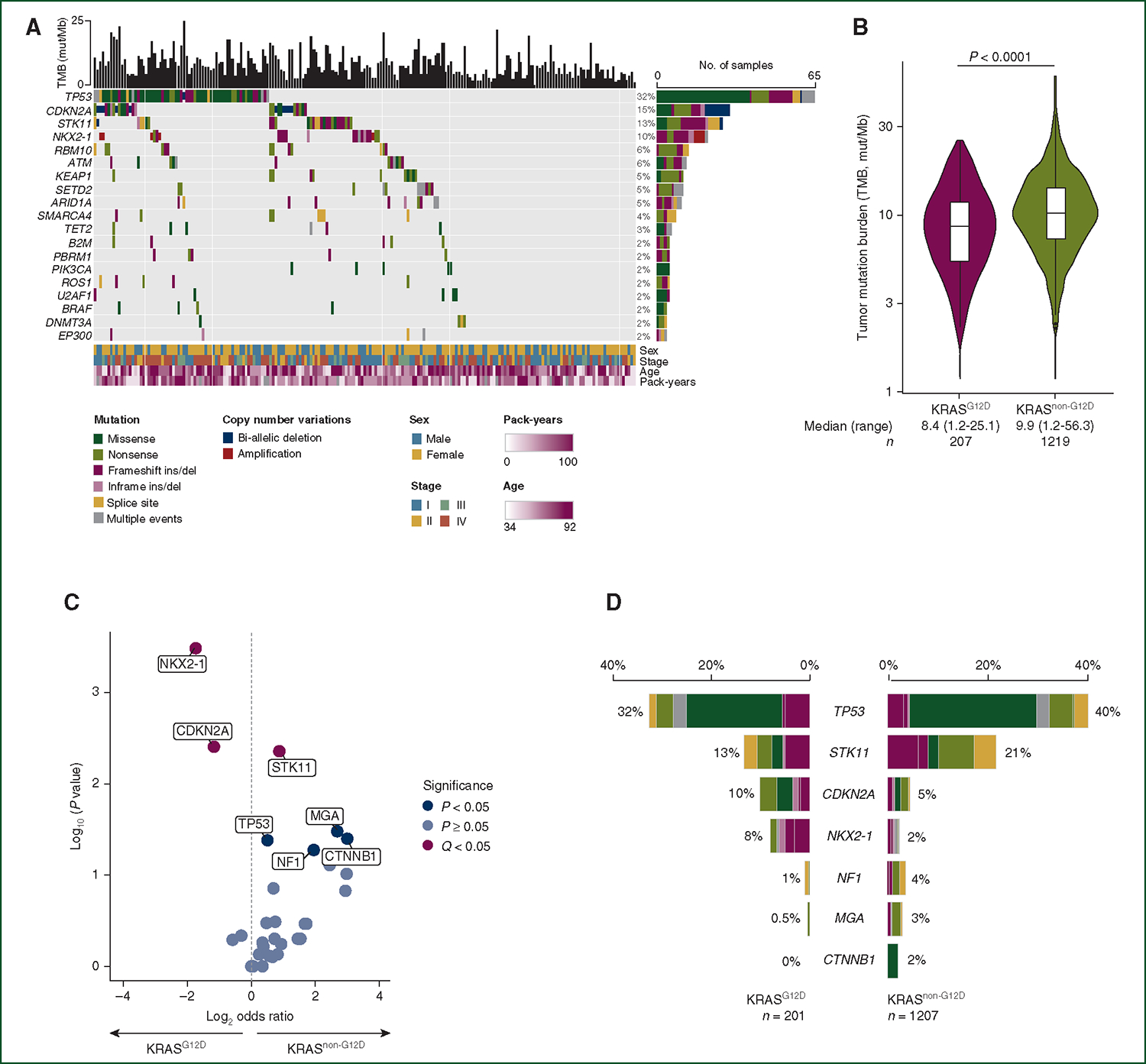
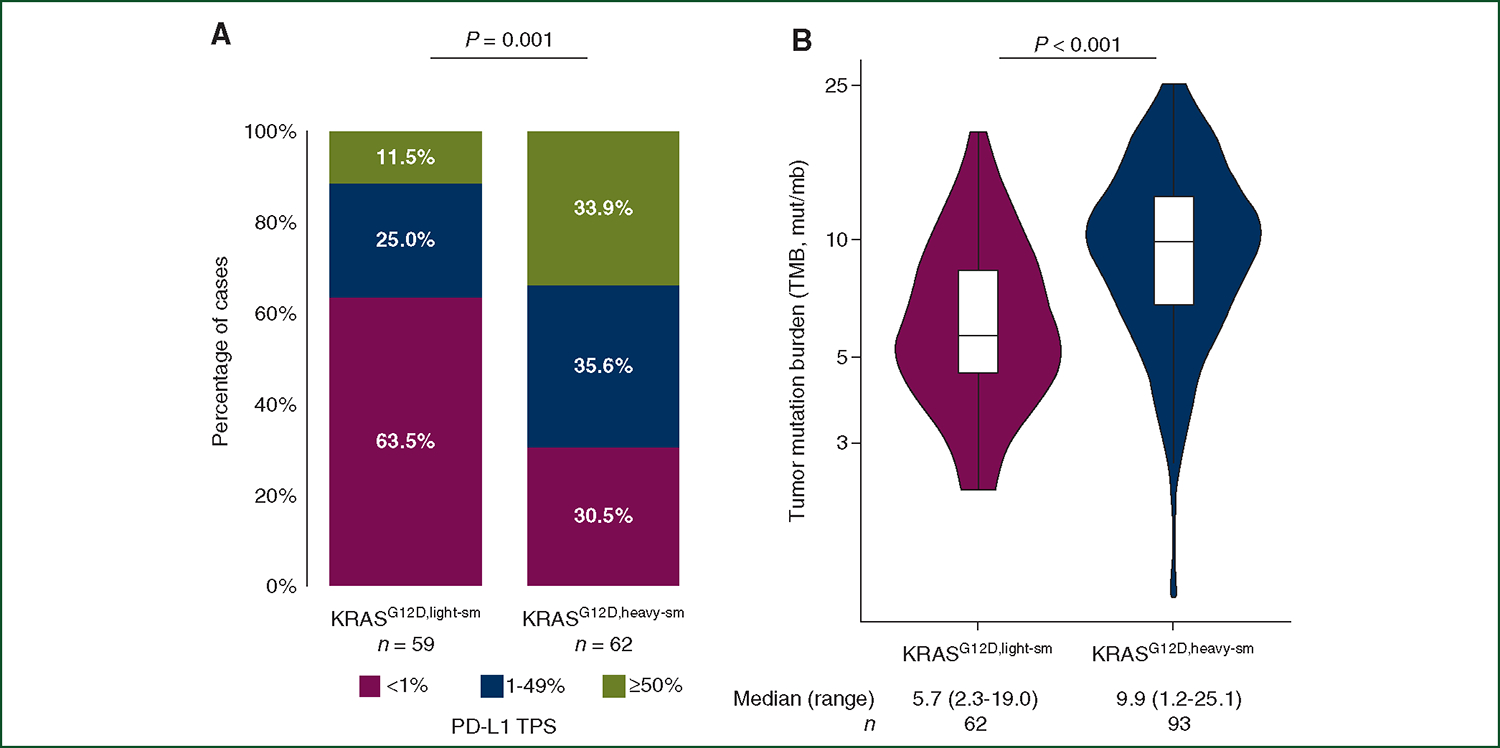
Of 2327 patients with KRAS-mutated (KRAS) NSCLC, 15% (n = 354) harbored KRAS. Compared to KRAS NSCLC, KRAS NSCLC had a lower pack-year (py) smoking history (median 22.5 py versus 30.0 py, P < 0.0001) and was enriched in never smokers (22% versus 5%, P < 0.0001). KRAS had lower PD-L1 tumor proportion score (TPS) (median 1% versus 5%, P < 0.01) and lower tumor mutation burden (TMB) compared to KRAS (median 8.4 versus 9.9 mt/Mb, P < 0.0001). Of the samples which underwent multiplexed immunofluorescence, KRAS had lower intratumoral and total CD8PD1 T cells (P < 0.05). Among 850 patients with advanced KRAS NSCLC who received PD-(L)1-based therapies, KRAS was associated with a worse objective response rate (ORR) (15.8% versus 28.4%, P = 0.03), progression-free survival (PFS) [hazard ratio (HR) 1.51, 95% confidence interval (CI) 1.45-2.00, P = 0.003], and overall survival (OS; HR 1.45, 1.05-1.99, P = 0.02) to PD-(L)1 inhibition alone but not to chemo-immunotherapy combinations [ORR 30.6% versus 35.7%, P = 0.51; PFS HR 1.28 (95%CI 0.92-1.77), P = 0.13; OS HR 1.36 (95%CI 0.95-1.96), P = 0.09] compared to KRAS.
KRAS lung cancers harbor distinct clinical, genomic, and immunologic features compared to other KRAS-mutated lung cancers and worse outcomes to PD-(L)1 blockade. Drug development for KRAS lung cancers will have to take these differences into account.
等位基因特异性 KRAS 抑制剂是一类新兴的癌症治疗药物。KRAS 突变(KRAS)非小细胞肺癌(NSCLC)的表现结果存在异质性,这是由不同的基础生物学差异导致的,这些差异是由共突变形成的。与 KRAS NSCLC 不同,KRAS NSCLC 与低/从不吸烟状态相关,且其特征在很大程度上尚未被描述。
在达纳-法伯癌症研究所(DFCI)、纪念斯隆凯特琳癌症中心、MD 安德森癌症中心和伦敦帝国理工学院,收集了携带 KRAS 突变的 NSCLC 患者的临床病理和基因组信息。在 DFCI 对部分有组织样本的患者进行了 CK7、程序性细胞死亡蛋白 1(PD-1)、程序性死亡配体 1(PD-L1)、Foxp3 和 CD8 的多重免疫荧光检测。根据 KRAS 突变亚型分析了 PD-(L)1 抑制联合/不联合化疗的临床结局。
在 2327 例 KRAS 突变(KRAS)NSCLC 患者中,15%(n=354)存在 KRAS 突变。与 KRAS NSCLC 相比,KRAS NSCLC 患者的吸烟史较短(中位 22.5 吸烟年数[py]与 30.0 py,P<0.0001),从不吸烟者比例更高(22%与 5%,P<0.0001)。与 KRAS 相比,KRAS 的 PD-L1 肿瘤比例评分(TPS)较低(中位 1%与 5%,P<0.01),肿瘤突变负荷(TMB)较低(中位 8.4 与 9.9 mt/Mb,P<0.0001)。在接受多重免疫荧光检测的样本中,KRAS 的肿瘤内和总 CD8PD1 T 细胞较少(P<0.05)。在 850 例接受 PD-(L)1 治疗的晚期 KRAS NSCLC 患者中,KRAS 与客观缓解率(ORR)更差(15.8%与 28.4%,P=0.03)、无进展生存期(PFS)[风险比(HR)1.51,95%置信区间(CI)1.45-2.00,P=0.003]和总生存期(OS;HR 1.45,1.05-1.99,P=0.02)更差,但与化疗免疫治疗联合治疗相比,无差异[ORR 30.6%与 35.7%,P=0.51;PFS HR 1.28(95%CI 0.92-1.77),P=0.13;OS HR 1.36(95%CI 0.95-1.96),P=0.09]。
与其他 KRAS 突变的 NSCLC 相比,KRAS 肺癌具有明显不同的临床、基因组和免疫学特征,且对 PD-(L)1 阻断的反应较差。针对 KRAS 肺癌的药物开发必须考虑到这些差异。