Department of Anaesthesiology, University of Duesseldorf, Duesseldorf, Germany.
L Boltzmann Institute for Traumatology in Cooperation with AUVA and Austrian Cluster for Tissue Regeneration, Vienna, Austria.
Front Immunol. 2022 Jul 7;13:895100. doi: 10.3389/fimmu.2022.895100. eCollection 2022.
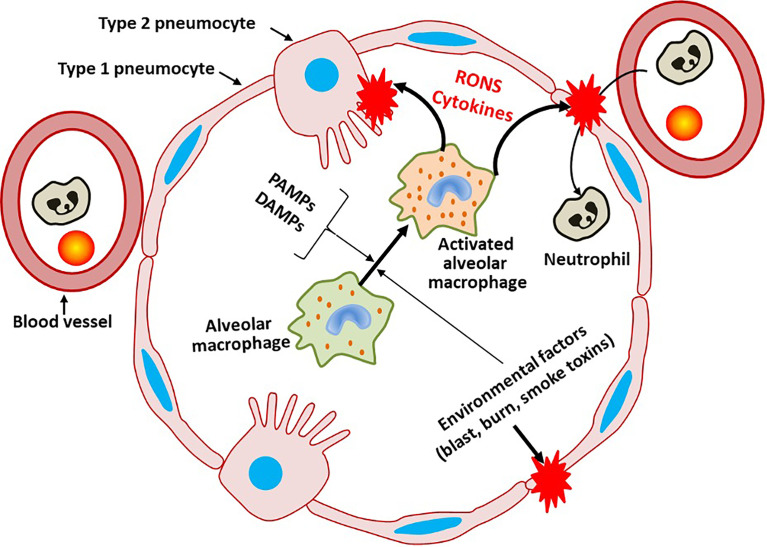
Pulmonary diseases represent four out of ten most common causes for worldwide mortality. Thus, pulmonary infections with subsequent inflammatory responses represent a major public health concern. The pulmonary barrier is a vulnerable entry site for several stress factors, including pathogens such as viruses, and bacteria, but also environmental factors e.g. toxins, air pollutants, as well as allergens. These pathogens or pathogen-associated molecular pattern and inflammatory agents e.g. damage-associated molecular pattern cause significant disturbances in the pulmonary barrier. The physiological and biological functions, as well as the architecture and homeostatic maintenance of the pulmonary barrier are highly complex. The airway epithelium, denoting the first pulmonary barrier, encompasses cells releasing a plethora of chemokines and cytokines, and is further covered with a mucus layer containing antimicrobial peptides, which are responsible for the pathogen clearance. Submucosal antigen-presenting cells and neutrophilic granulocytes are also involved in the defense mechanisms and counterregulation of pulmonary infections, and thus may directly affect the pulmonary barrier function. The detailed understanding of the pulmonary barrier including its architecture and functions is crucial for the diagnosis, prognosis, and therapeutic treatment strategies of pulmonary diseases. Thus, considering multiple side effects and limited efficacy of current therapeutic treatment strategies in patients with inflammatory diseases make experimental and models necessary to improving clinical therapy options. This review describes existing models for studyying the pulmonary barrier function under acute inflammatory conditions, which are meant to improve the translational approaches for outcome predictions, patient monitoring, and treatment decision-making.
肺部疾病占全球十大死亡原因中的四项。因此,肺部感染及其后续的炎症反应是一个主要的公共卫生关注点。肺部屏障是多种应激因素(包括病毒和细菌等病原体,以及毒素、空气污染物和过敏原等环境因素)进入人体的脆弱部位。这些病原体或病原体相关的分子模式和炎症介质,如损伤相关分子模式,会导致肺部屏障的显著紊乱。肺部屏障的生理和生物学功能、结构和稳态维持非常复杂。气道上皮作为第一道肺部屏障,包含释放大量趋化因子和细胞因子的细胞,进一步被含有抗菌肽的黏液层覆盖,这些细胞和物质负责清除病原体。黏膜下抗原呈递细胞和嗜中性粒细胞也参与肺部感染的防御机制和反向调节,因此可能直接影响肺部屏障功能。详细了解肺部屏障的结构和功能对于肺部疾病的诊断、预后和治疗策略至关重要。因此,考虑到炎症性疾病患者当前治疗策略的多种副作用和有限疗效,实验和模型对于改善临床治疗选择是必要的。本综述描述了研究急性炎症条件下肺部屏障功能的现有模型,旨在改进用于预测结果、患者监测和治疗决策的转化方法。