Division of Bone Marrow Transplantation and Immune Deficiency, Cancer and Blood Diseases Institute, Cincinnati Children's Hospital Medical Center, Cincinnati, OH.
Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH; and.
Blood Adv. 2022 Jul 26;6(14):4310-4319. doi: 10.1182/bloodadvances.2022007453.
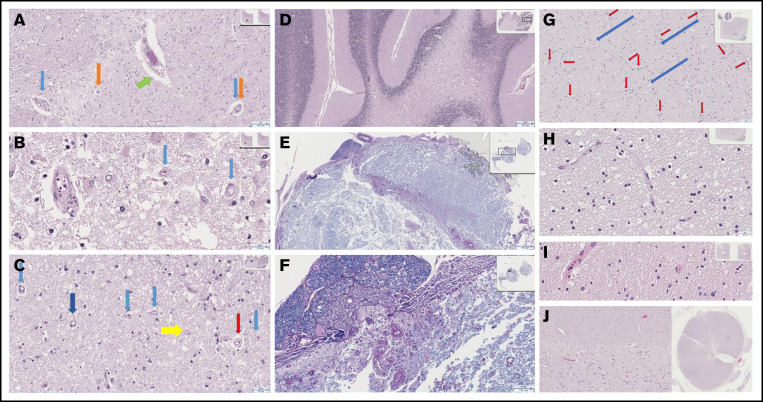
Transplant-associated thrombotic microangiopathy (TA-TMA) and atypical hemolytic uremic syndrome (aHUS) are complement-mediated TMAs. The central nervous system (CNS) is the most common extrarenal organ affected by aHUS, and, despite mechanistic overlap between aHUS and TA-TMA, CNS involvement is rarely reported in TA-TMA, suggesting that CNS involvement in TA-TMA may be underdiagnosed and that these patients may benefit from complement blockers. In addition, there are no widely used histologic or radiologic criteria for the diagnosis of TMA in the brain. Thirteen recipients of pediatric hematopoietic cell transplants (HCTs) who had TA-TMA and who underwent autopsy were studied. Seven of 13 brains had vascular injury, and 2 had severe vascular injury. Neurologic symptoms correlated with severe vascular injury. Classic TMA histology was present and most often observed in the cerebellum, brainstem, and cerebral white matter. Abnormalities in similar anatomic regions were seen on imaging. Brain imaging findings related to TMA included hemorrhages, siderosis, and posterior reversible encephalopathy syndrome. We then studied 100 consecutive HCT recipients to identify differences in neurologic complications between patients with and those without TA-TMA. Patients with TA-TMA were significantly more likely to have a clinical concern for seizure, have an electroencephalogram performed, and develop altered mental status. In summary, our study confirms that TA-TMA involves the brains of recipients of HCT and is associated with an increased incidence of neurologic symptoms. Based on these findings, we propose that patients with low- or moderate-risk TA-TMA who develop neurologic complications should be considered for TA-TMA-directed therapy.
移植相关血栓性微血管病(TA-TMA)和非典型溶血尿毒症综合征(aHUS)是补体介导的 TMA。中枢神经系统(CNS)是 aHUS 最常累及的肾外器官,尽管 aHUS 和 TA-TMA 之间存在机制重叠,但 TA-TMA 中 CNS 受累很少见,这表明 TA-TMA 中的 CNS 受累可能被漏诊,这些患者可能受益于补体抑制剂。此外,目前尚无用于诊断大脑 TMA 的广泛使用的组织学或影像学标准。研究了 13 名接受儿科造血细胞移植(HCT)的 TA-TMA 患者,并对其进行了尸检。在 13 例大脑中,有 7 例存在血管损伤,2 例存在严重血管损伤。神经症状与严重血管损伤相关。经典的 TMA 组织学存在,最常观察到小脑、脑干和大脑白质。在影像学上也观察到类似的解剖区域存在异常。与 TMA 相关的脑影像学表现包括出血、含铁血黄素沉着和后部可逆性脑病综合征。然后,我们研究了 100 名连续 HCT 受者,以确定 TMA 患者和非 TMA 患者之间神经并发症的差异。患有 TA-TMA 的患者更有可能出现癫痫发作的临床关注,进行脑电图检查,并出现精神状态改变。总之,我们的研究证实 TA-TMA 涉及 HCT 受者的大脑,并与神经症状发生率增加有关。基于这些发现,我们建议对出现神经并发症的低危或中危 TA-TMA 患者应考虑进行 TA-TMA 靶向治疗。