Faculty of Medicine, School of Public Health-University of Vita-Salute San Raffaele, Milano, Italy.
Department of Research and Development, Agenzia Regionale Emergenza Urgenza Headquarters (AREU HQ), Milano, Italy.
Acta Anaesthesiol Scand. 2022 Oct;66(9):1124-1129. doi: 10.1111/aas.14117. Epub 2022 Aug 5.
The coronavirus disease 2019 (COVID-19) pandemic changed the time-dependent cardiac arrest network. This study aims to understand whether the rescue standards of cardiopulmonary resuscitation (CPR) and out-of-hospital cardiac arrest (OHCA) were handled differently during pandemic compared to the previous year.
Data for the years 2019 and 2020 were provided by the records of the Lombardy office of the Regional Agency for Emergency and Urgency. We analysed where the cardiac arrest occurred, when CPR started and whether the bystanders used public access to defibrillation (PAD).
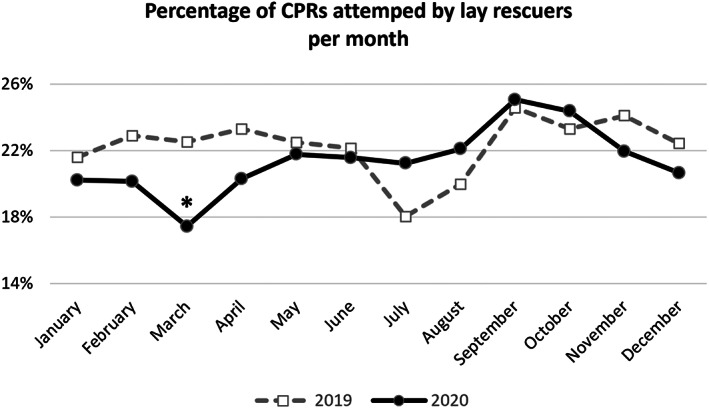
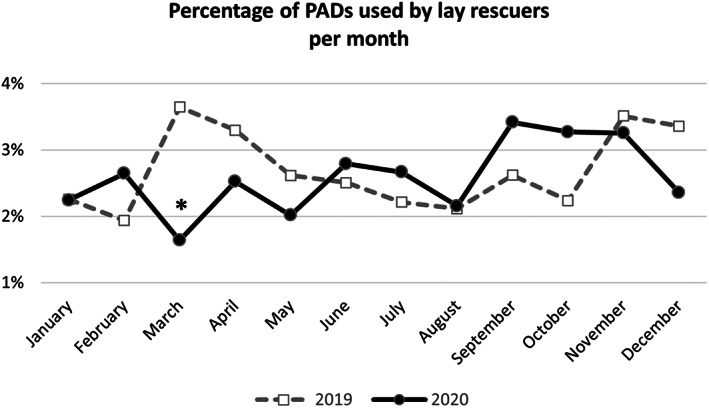
During 2020, there was a reduction in CPRs performed by bystanders (odds ratio [OR] = 0.936 [95% confidence interval (CI ) 0.882-0.993], p = .029) and in the return of spontaneous circulation (ROSC) (OR = 0.621 [CI 0.563-0.685], p < .0001), while there was no significant reduction in the use of PAD. Analysing only March, the period of the first wave in Lombardy, the comparison shows a reduction in bystanders CPRs (OR = 0.727 [CI 0.602-0.877], p = .0008), use of PAD (OR = 0.441 [CI 0.272-0.716], p = .0009) and in ROSC (OR = 0.179 [CI 0.124-0.257], p < .0001). These phenomena could be influenced by the different settings in which the OHCAs occurred; in fact, those that occurred in public places with a mandatory PAD were strongly reduced (OR = 0.49 [CI , 0.44-0.55], p < .0001).
COVID-19 had a profound impact on the time-dependant OHCA network. During the first pandemic wave, CPR and PAD used by bystanders decreased. The different contexts in which OHCAs occurred may partially explain these differences.
2019 年冠状病毒病(COVID-19)大流行改变了时间依赖型心脏骤停网络。本研究旨在了解与前一年相比,大流行期间心肺复苏(CPR)和院外心脏骤停(OHCA)的抢救标准是否有所不同。
提供了 2019 年和 2020 年的数据,这些数据来自伦巴第地区紧急和紧急事务处的记录。我们分析了心脏骤停发生的地点、CPR 开始的时间以及旁观者是否使用公共获取除颤器(PAD)。
2020 年,旁观者实施的 CPR(优势比[OR] = 0.936 [95%置信区间(CI)0.882-0.993],p = 0.029)和自主循环恢复(ROSC)(OR = 0.621 [CI 0.563-0.685],p < 0.0001)减少,而 PAD 的使用并未显著减少。仅分析伦巴第第一波的 3 月期间,比较显示旁观者 CPR 减少(OR = 0.727 [CI 0.602-0.877],p = 0.0008),PAD 使用率(OR = 0.441 [CI 0.272-0.716],p = 0.0009)和 ROSC(OR = 0.179 [CI 0.124-0.257],p < 0.0001)。这些现象可能受到 OHCA 发生地点不同的影响;事实上,在公共场所强制使用 PAD 的 OHCA 明显减少(OR = 0.49 [CI 0.44-0.55],p < 0.0001)。
COVID-19 对时间依赖型 OHCA 网络产生了深远影响。在第一波大流行期间,旁观者实施的 CPR 和 PAD 减少。OHCA 发生的不同环境可能部分解释了这些差异。