Owen Andrew, Patel Jaimin M, Parekh Dhruv, Bangash Mansoor N
Department of Critical Care, Queen Elizabeth Hospital, University Hospitals Birmingham, Birmingham, United Kingdom.
Birmingham Acute Care Research Group, Institute of Inflammation and Ageing, University of Birmingham, Birmingham, United Kingdom.
Front Cardiovasc Med. 2022 Jul 15;9:854421. doi: 10.3389/fcvm.2022.854421. eCollection 2022.
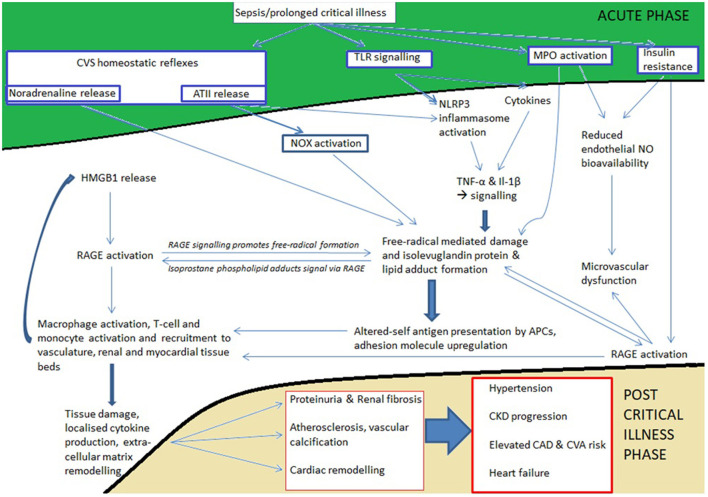
Prolonged critical care stays commonly follow trauma, severe burn injury, sepsis, ARDS, and complications of major surgery. Although patients leave critical care following homeostatic recovery, significant additional diseases affect these patients during and beyond the convalescent phase. New cardiovascular and renal disease is commonly seen and roughly one third of all deaths in the year following discharge from critical care may come from this cluster of diseases. During prolonged critical care stays, the immunometabolic, inflammatory and neurohumoral response to severe illness in conjunction with resuscitative treatments primes the immune system and parenchymal tissues to develop a long-lived pro-inflammatory and immunosenescent state. This state is perpetuated by persistent Toll-like receptor signaling, free radical mediated isolevuglandin protein adduct formation and presentation by antigen presenting cells, abnormal circulating HDL and LDL isoforms, redox and metabolite mediated epigenetic reprogramming of the innate immune arm (trained immunity), and the development of immunosenescence through T-cell exhaustion/anergy through epigenetic modification of the T-cell genome. Under this state, tissue remodeling in the vascular, cardiac, and renal parenchymal beds occurs through the activation of pro-fibrotic cellular signaling pathways, causing vascular dysfunction and atherosclerosis, adverse cardiac remodeling and dysfunction, and proteinuria and accelerated chronic kidney disease.
长时间的重症监护通常发生在创伤、严重烧伤、败血症、急性呼吸窘迫综合征(ARDS)以及大手术并发症之后。尽管患者在恢复内环境稳定后离开重症监护病房,但在康复期及康复期之后,仍有其他严重疾病影响这些患者。常见的有新发心血管和肾脏疾病,在从重症监护病房出院后的一年内,所有死亡病例中约有三分之一可能源于这一系列疾病。在长时间的重症监护期间,对重症疾病的免疫代谢、炎症和神经体液反应,再加上复苏治疗,会使免疫系统和实质组织进入一种长期存在的促炎和免疫衰老状态。这种状态通过持续的Toll样受体信号传导、自由基介导的异前列腺素蛋白加合物形成及抗原呈递细胞的呈递、循环中异常的高密度脂蛋白(HDL)和低密度脂蛋白(LDL)亚型、氧化还原和代谢物介导的固有免疫臂(训练免疫)的表观遗传重编程,以及通过T细胞基因组的表观遗传修饰导致T细胞耗竭/无反应性而产生免疫衰老得以持续。在这种状态下,血管、心脏和肾脏实质床的组织重塑通过促纤维化细胞信号通路的激活而发生,导致血管功能障碍和动脉粥样硬化、不良心脏重塑和功能障碍,以及蛋白尿和慢性肾脏病加速进展。