Koegelenberg C F N, van Zyl-Smit R N, Dheda K, Allwood B W, Vorster M J, Plekker D, Slebos D-J, Klooster K, Shah P L, Herth F J F
Division of Pulmonology, Department of Medicine, Stellenbosch University and Tygerberg Academic Hospital, Cape Town, South Africa.
Division of Pulmonology, Department of Medicine, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa.
Afr J Thorac Crit Care Med. 2022 Jun 20;28(2). doi: 10.7196/AJTCCM.2022.v28i2.249. eCollection 2022.
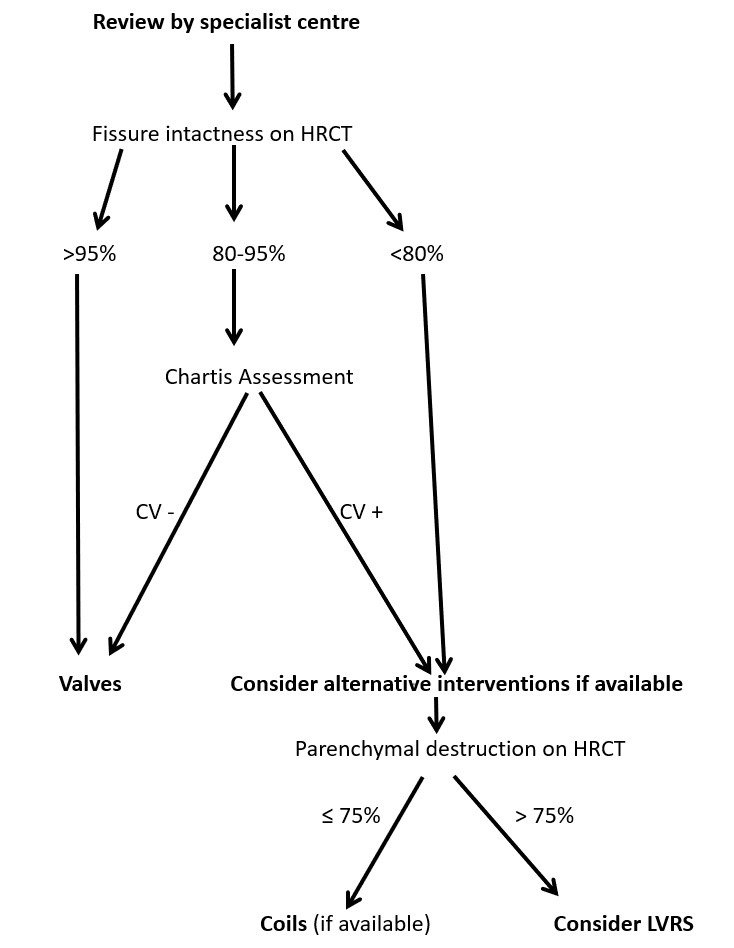
Chronic obstructive pulmonary disease (COPD) remains one of the most common causes of morbidity and mortality in South Africa. Endoscopic lung volume reduction (ELVR) was first proposed by the South African Thoracic Society (SATS) for the treatment of advanced emphysema in 2015. Since the original statement was published, there has been a growing body of evidence that a certain well-defined sub-group of patients with advanced emphysema may benefit from ELVR, to the point where the current Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines and the United Kingdom National Institute for Health and Care Excellence (NICE) advocate the use of endoscopic valves based on level A evidence. Patients aged 40 - 75 years with severe dyspnoea (COPD Assessment Test score ≥10) despite maximal medical therapy and pulmonary rehabilitation, with forced expiratory volume in one second (FEV) 20 - 50%, hyperinflation with residual volume (RV) >175% or RV/total lung capacity (TLC) >55% and a six-minute walking distance (6MWD) of 100 - 450 m (post-rehabilitation) should be referred for evaluation for ELVR, provided no contraindications (e.g. severe pulmonary hypertension) are present. Further evaluation should focus on the extent of parenchymal tissue destruction on high-resolution computed tomography (HRCT) of the lungs and interlobar collateral ventilation (CV) to identify a potential target lobe. Commercially available radiology software packages and/or an endobronchial catheter system can aid in this assessment. The aim of this statement is to provide the South African medical practitioner and healthcare funders with an overview of the practical aspects and current evidence for the judicious use of the valves and other ELVR modalities which may become available in the country.
慢性阻塞性肺疾病(COPD)仍是南非发病和死亡的最常见原因之一。2015年,南非胸科学会(SATS)首次提出采用内镜下肺减容术(ELVR)治疗晚期肺气肿。自最初声明发表以来,越来越多的证据表明,某一明确界定的晚期肺气肿亚组患者可能从ELVR中获益,以至于目前的全球慢性阻塞性肺疾病倡议(GOLD)指南和英国国家卫生与临床优化研究所(NICE)基于A级证据提倡使用内镜瓣膜。年龄在40 - 75岁、尽管接受了最大程度的药物治疗和肺康复仍有严重呼吸困难(慢性阻塞性肺疾病评估测试评分≥10)、一秒用力呼气量(FEV)为20 - 50%、存在肺过度充气且残气量(RV)>175%或RV/肺总量(TLC)>55%以及六分钟步行距离(6MWD)为100 - 450米(康复后)的患者,若不存在禁忌证(如严重肺动脉高压),应转诊接受ELVR评估。进一步评估应侧重于肺部高分辨率计算机断层扫描(HRCT)上实质组织破坏的程度以及叶间侧支通气(CV),以确定潜在的目标肺叶。市售的放射学软件包和/或支气管内导管系统有助于此项评估。本声明的目的是向南非的医生和医疗保健资助者概述该国可能会有的瓣膜及其他ELVR方式合理使用的实际情况和当前证据。