Gálvez-Sirvent Elena, Ibarzábal-Gil Aitor, Rodríguez-Merchán E Carlos
Department of Orthopaedic Surgery, "Infanta Elena" University Hospital, Valdemoro, Madrid, Spain.
Faculty of Medicine, Universidad Francisco de Vitoria, Madrid, Spain.
EFORT Open Rev. 2022 Aug 4;7(8):554-568. doi: 10.1530/EOR-22-0004.
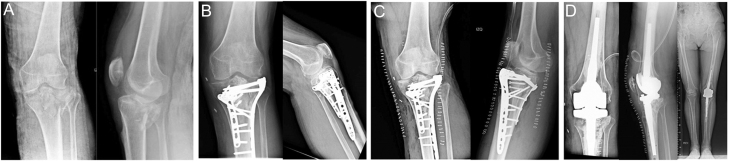
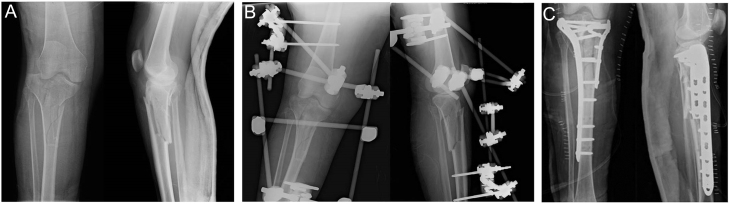
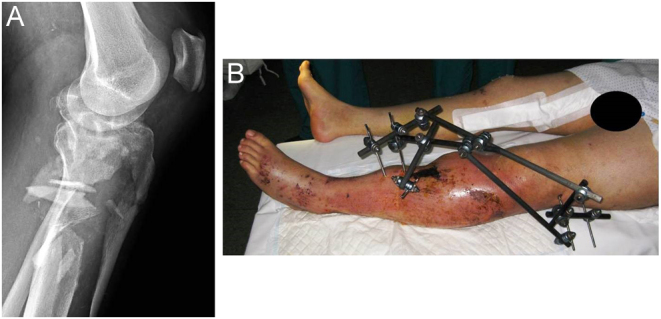
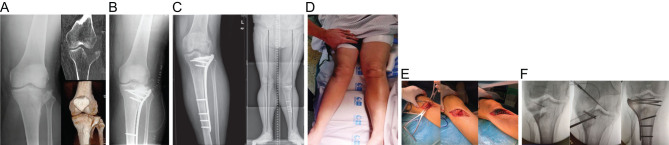
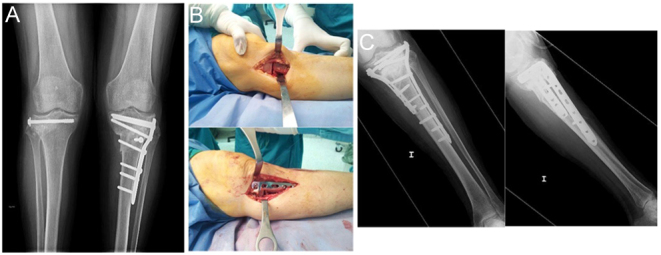
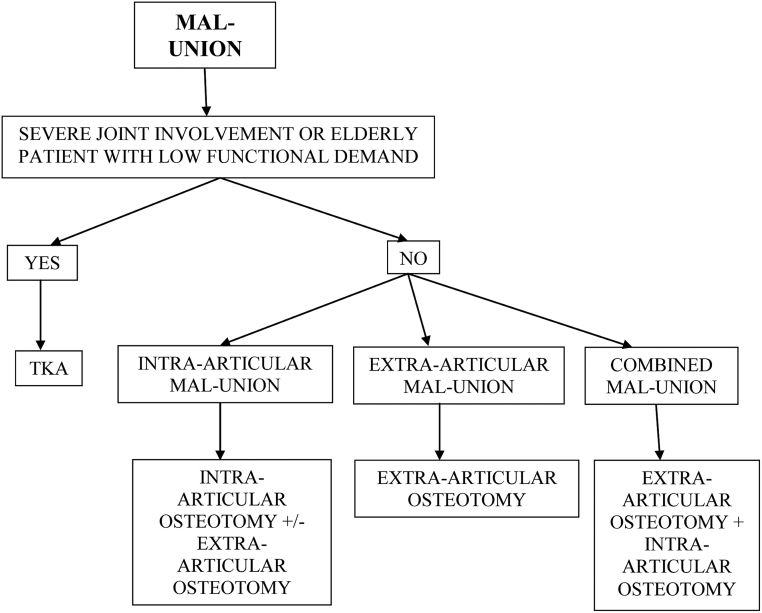
Open reduction and internal fixation is the gold standard treatment for tibial plateau fractures. However, the procedure is not free of complications such as knee stiffness, acute infection, chronic infection (osteomyelitis), malunion, non-union, and post-traumatic osteoarthritis. The treatment options for knee stiffness are mobilisation under anaesthesia (MUA) when the duration is less than 3 months, arthroscopic release when the duration is between 3 and 6 months, and open release for refractory cases or cases lasting more than 6 months. Early arthroscopic release can be associated with MUA. Regarding treatment of acute infection, if the fracture has healed, the hardware can be removed, and lavage and debridement can be performed along with antibiotic therapy. If the fracture has not healed, the hardware is retained, and lavage, debridement, and antibiotic therapy are performed (sometimes more than once until the fracture heals). Fracture stability is important not only for healing but also for resolving the infection. In cases of osteomyelitis, treatment should be performed in stages: aggressive debridement of devitalised tissue and bone, antibiotic spacing and temporary external fixation until the infection is resolved (first stage), followed by definitive surgery with grafting or soft tissue coverage depending on the bone defect (second stage). Intra-articular or extra-articular osteotomy is a good option to correct malunion in young, active patients without significant joint damage. When malunion is associated with extensive joint involvement or the initial cartilage damage has resulted in knee osteoarthritis, the surgical option is total knee arthroplasty.
切开复位内固定是胫骨平台骨折的金标准治疗方法。然而,该手术并非没有并发症,如膝关节僵硬、急性感染、慢性感染(骨髓炎)、骨不连、骨不愈合以及创伤后骨关节炎。对于膝关节僵硬的治疗选择如下:病程小于3个月时采用麻醉下手法松解(MUA),病程在3至6个月之间时采用关节镜下松解,对于难治性病例或病程超过6个月的病例采用切开松解。早期关节镜下松解可与MUA联合使用。关于急性感染的治疗,如果骨折已愈合,可取出内固定物,并在抗生素治疗的同时进行冲洗和清创。如果骨折未愈合,则保留内固定物,并进行冲洗、清创和抗生素治疗(有时需多次进行直至骨折愈合)。骨折稳定性不仅对愈合很重要,对解决感染也很重要。对于骨髓炎病例,治疗应分阶段进行:积极清创失活组织和骨组织,进行抗生素间隔治疗并临时外固定直至感染得到解决(第一阶段),随后根据骨缺损情况进行确定性手术,采用植骨或软组织覆盖(第二阶段)。对于年轻、活跃且关节无明显损伤的患者,关节内或关节外截骨术是纠正骨不连的良好选择。当骨不连伴有广泛的关节受累或初始软骨损伤导致膝关节骨关节炎时,手术选择是全膝关节置换术。