Department of Communication Sciences and Disorders, University of South Carolina, Columbia, SC, USA.
Department of Communication Sciences and Disorders, University of South Carolina, Columbia, SC, USA.
Cortex. 2022 Sep;154:375-389. doi: 10.1016/j.cortex.2022.06.013. Epub 2022 Jul 8.
Lesion-related factors are associated with severity of language impairment in persons with aphasia. The extent to which demographic and health factors predict language impairment beyond traditional cortical measures remains unknown. Identifying and understanding the contributions of factors to predictive models of severity constitutes critical knowledge for clinicians interested in charting the likely course of aphasia in their patients and designing effective treatment approaches in light of those predictions.
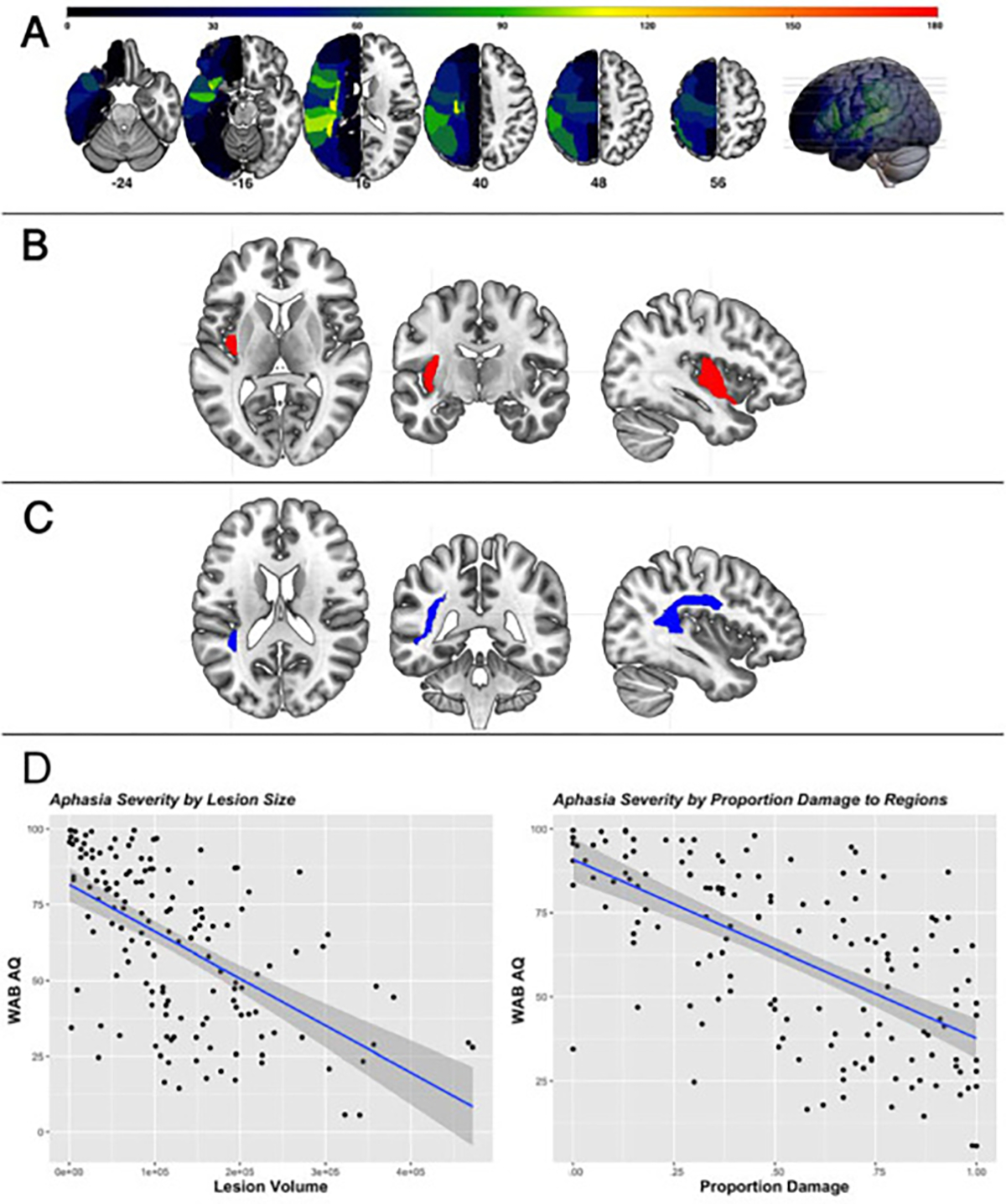
Utilizing neuroimaging and language testing from our cohort of 224 individuals in the chronic stage of recovery from a left-hemisphere stroke in a cross-sectional study, we first conducted a lesion symptom mapping (LSM) analysis to identify regions associated with aphasia severity scores. After controlling for lesion volume and damage to pre-identified areas, three models were created to predict severity scores: 1) Demographic Model (N = 147); 2) Health Model (N = 106); and 3) Overall Model (N = 106). Finally, all identified factors were entered into a Final Model to predict raw severity scores.
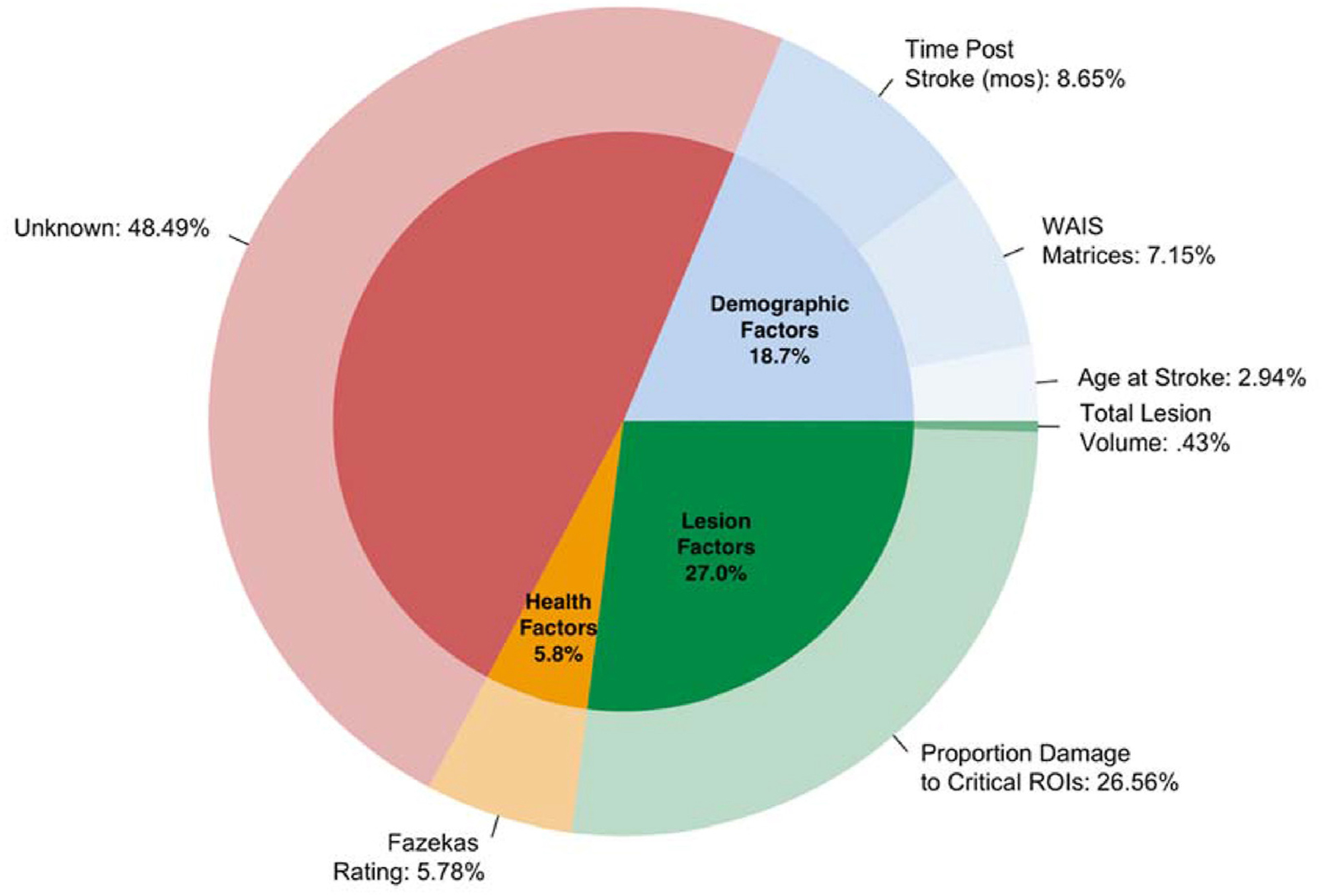
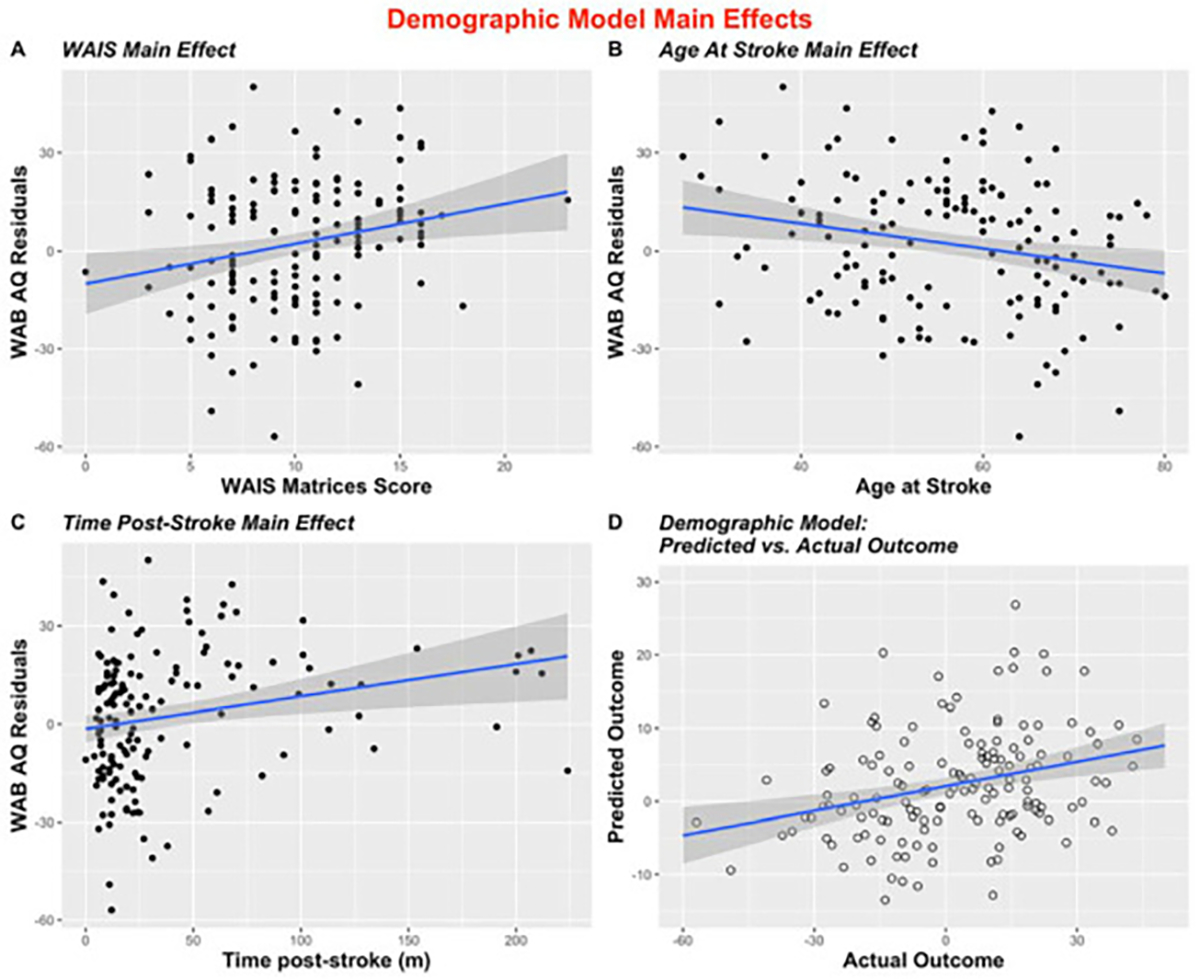
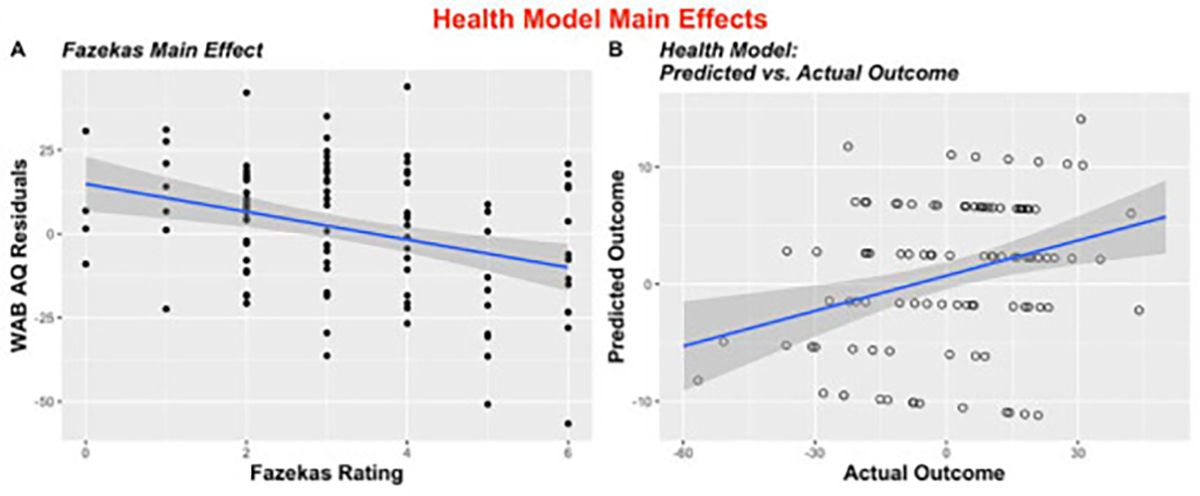
Two areas were associated with aphasia severity-left posterior insula and left arcuate fasciculus. The results from the Demographic Model revealed non-linguistic cognitive ability, age at stroke, and time post-stroke as significant predictors of severity (P = .005; P = .02; P = .001, respectively), and results from the Health Model suggested the extent of leukoaraiosis is associated with severity (P = .0004). The Overall Model showed a relationship between aphasia severity and cognitive ability (P = .01), time post-stroke (P = .002), and leukoaraiosis (P = .01). In the Final Model, which aimed to predict raw severity scores, demographic, health, and lesion factors explained 55% of the variance in severity, with health and demographic factors uniquely explaining nearly half of performance variance.
Results from this study add to the literature suggesting patient-specific variables can shed light on individual differences in severity beyond lesion factors. Additionally, our results emphasize the importance of non-linguistic cognitive ability and brain health in aphasia recovery.
病灶相关因素与失语症患者语言障碍的严重程度有关。在传统皮质测量之外,人口统计学和健康因素在多大程度上可以预测语言障碍仍不得而知。确定和理解这些因素对严重程度预测模型的贡献,对于有兴趣了解患者失语症可能进程并根据这些预测制定有效治疗方法的临床医生来说,是至关重要的知识。
在一项横断面研究中,我们利用来自 224 名左侧大脑半球卒中后慢性期患者的神经影像学和语言测试数据,首先进行了病灶症状映射(LSM)分析,以确定与失语症严重程度评分相关的区域。在控制病灶体积和预先确定区域的损伤后,我们创建了三个模型来预测严重程度评分:1)人口统计学模型(N=147);2)健康模型(N=106);3)总体模型(N=106)。最后,将所有确定的因素纳入最终模型,以预测原始严重程度评分。
两个区域与失语症严重程度相关——左侧后岛叶和左侧弓状束。人口统计学模型的结果显示,非语言认知能力、卒中时年龄和卒中后时间是严重程度的显著预测因素(P=0.005;P=0.02;P=0.001),健康模型的结果表明白质疏松的程度与严重程度相关(P=0.0004)。总体模型显示,失语症严重程度与认知能力(P=0.01)、卒中后时间(P=0.002)和白质疏松(P=0.01)有关。在最终模型中,旨在预测原始严重程度评分,人口统计学、健康和病灶因素解释了严重程度方差的 55%,健康和人口统计学因素单独解释了近一半的表现方差。
本研究结果增加了文献资料,表明患者特定变量可以揭示病灶因素之外的严重程度的个体差异。此外,我们的结果强调了非语言认知能力和大脑健康在失语症康复中的重要性。