Malaria Research and Training Centre Ogobara K. Doumbo (MRTC-OKD), FMOS-FAPH, Mali-NIAID-ICER, Université Des Sciences, Des Techniques Et Des Technologies de Bamako, 1805, Bamako, Mali.
INSERM, IRD, ISSPAM, UM1252, Aix-Marseille University, 13005, Marseille, France.
Parasit Vectors. 2022 Aug 4;15(1):278. doi: 10.1186/s13071-022-05379-4.
In malaria endemic countries, seasonal malaria chemoprevention (SMC) interventions are performed during the high malaria transmission in accordance with epidemiological surveillance data. In this study we propose a predictive approach for tailoring the timing and number of cycles of SMC in all health districts of Mali based on sub-national epidemiological surveillance and rainfall data. Our primary objective was to select the best of two approaches for predicting the onset of the high transmission season at the operational scale. Our secondary objective was to evaluate the number of malaria cases, hospitalisations and deaths in children under 5 years of age that would be prevented annually and the additional cost that would be incurred using the best approach.
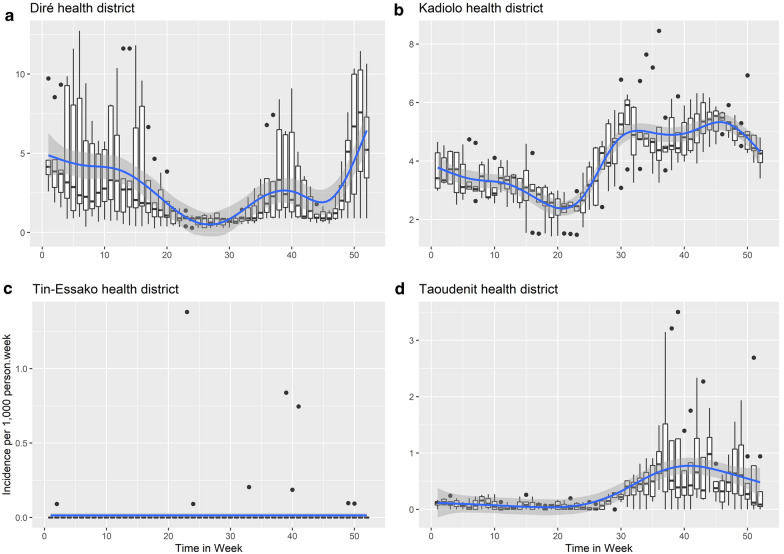
For each of the 75 health districts of Mali over the study period (2014-2019), we determined (1) the onset of the rainy season period based on weekly rainfall data; (ii) the onset and duration of the high transmission season using change point analysis of weekly incidence data; and (iii) the lag between the onset of the rainy season and the onset of the high transmission. Two approaches for predicting the onset of the high transmission season in 2019 were evaluated.
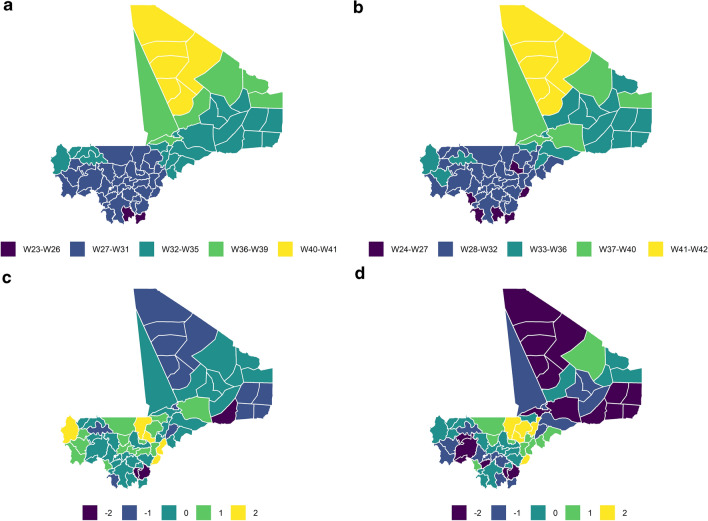
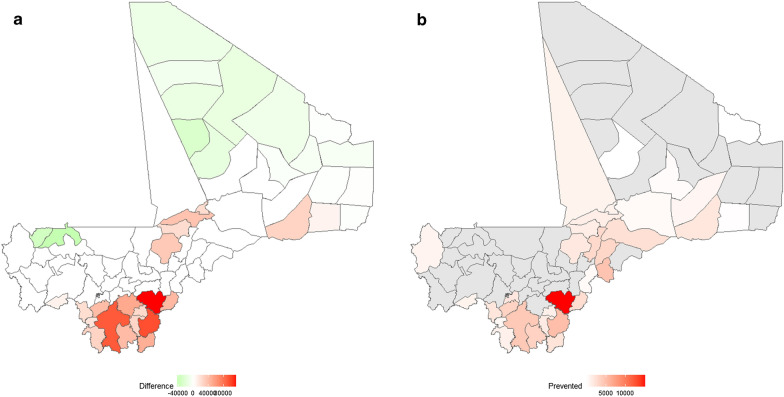
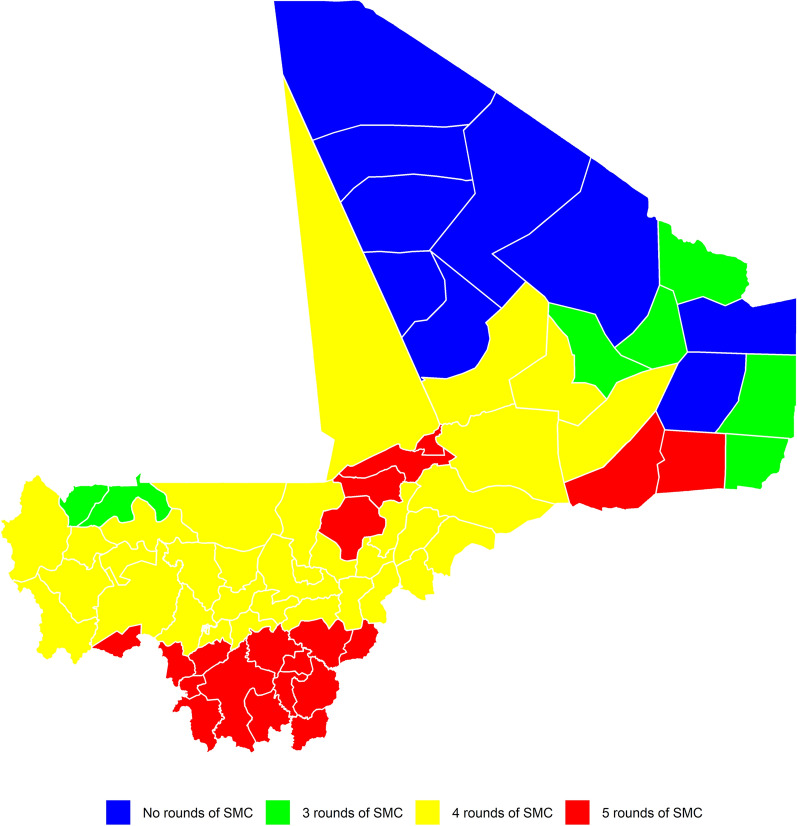
In the study period (2014-2019), the onset of the rainy season ranged from week (W) 17 (W17; April) to W34 (August). The onset of the high transmission season ranged from W25 (June) to W40 (September). The lag between these two events ranged from 5 to 12 weeks. The duration of the high transmission season ranged from 3 to 6 months. The best of the two approaches predicted the onset of the high transmission season in 2019 to be in June in two districts, in July in 46 districts, in August in 21 districts and in September in six districts. Using our proposed approach would prevent 43,819 cases, 1943 hospitalisations and 70 deaths in children under 5 years of age annually for a minimal additional cost. Our analysis shows that the number of cycles of SMC should be changed in 36 health districts.
Adapting the timing of SMC interventions using our proposed approach could improve the prevention of malaria cases and decrease hospitalisations and deaths. Future studies should be conducted to validate this approach.
在疟疾流行国家,根据流行病学监测数据,在疟疾高传播季节进行季节性疟疾化学预防(SMC)干预。在这项研究中,我们提出了一种基于次国家流行病学监测和降雨数据来定制马里所有卫生区 SMC 时间和周期的预测方法。我们的主要目标是选择两种方法中的最佳方法来预测高传播季节的开始,以实现操作规模。我们的次要目标是评估每年使用最佳方法预防 5 岁以下儿童疟疾病例、住院和死亡的数量,以及额外的成本。
在研究期间(2014-2019 年),对于马里的 75 个卫生区中的每一个,我们确定了:(1)根据每周降雨数据确定雨季开始的时间;(ii)使用每周发病率数据的变化点分析确定高传播季节的开始和持续时间;以及(iii)雨季开始和高传播季节开始之间的滞后时间。评估了两种预测 2019 年高传播季节开始的方法。
在研究期间(2014-2019 年),雨季开始的时间从第 17 周(W17;4 月)到第 34 周(8 月)不等。高传播季节的开始时间从第 25 周(6 月)到第 40 周(9 月)不等。这两个事件之间的滞后时间从 5 周到 12 周不等。高传播季节的持续时间从 3 个月到 6 个月不等。这两种方法中的最佳方法预测 2019 年高传播季节的开始时间在两个地区为 6 月,在 46 个地区为 7 月,在 21 个地区为 8 月,在 6 个地区为 9 月。使用我们建议的方法每年可预防 43819 例病例、1943 例住院和 70 例 5 岁以下儿童死亡,额外费用最小。我们的分析表明,应改变 36 个卫生区的 SMC 周期。
使用我们建议的方法调整 SMC 干预的时间可以提高预防疟疾病例的效果,并减少住院和死亡人数。未来的研究应验证这种方法。