Service de Cardiologie, Centre Hospitalier Universitaire Trousseau Faculté de Médecine, Université François Rabelais Tours France.
Service d'information médicale, d'épidémiologie et d'économie de la santé, Centre Hospitalier Universitaire et EA7505 Faculté de Médecine, Université François Rabelais Tours France.
J Am Heart Assoc. 2022 Aug 16;11(16):e025339. doi: 10.1161/JAHA.122.025339. Epub 2022 Aug 5.
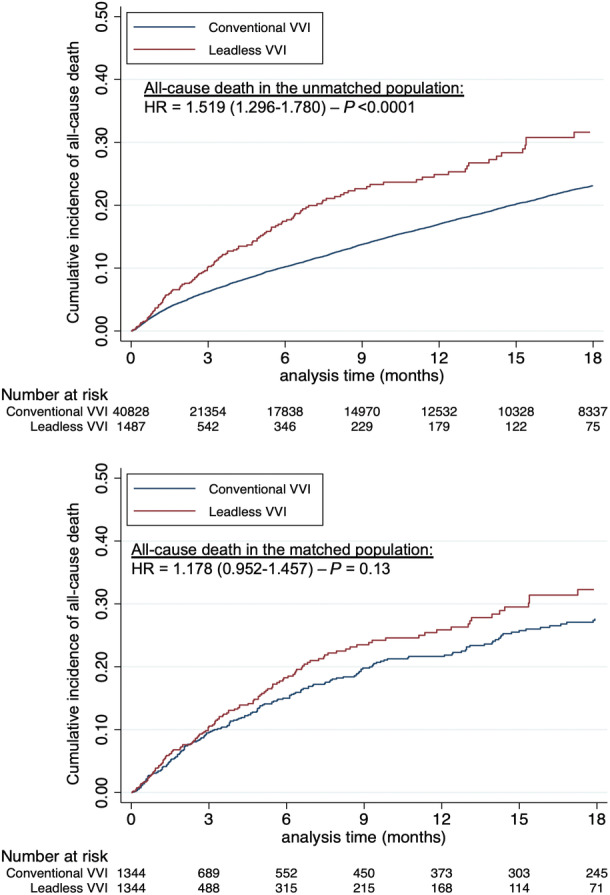
Background Leadless ventricular permanent pacemakers (leadless VVI or LPM) were designed to reduce lead-related complications of conventional VVI pacemakers (CPM). The aim of our study was to assess and compare real-life clinical outcomes within the first 30 days and during a midterm follow-up with the 2 techniques. Methods and Results This French longitudinal cohort study was based on the national hospitalization database. All adults (age ≥18 years) hospitalized in French hospitals from January 1, 2017 to September 1, 2020, who underwent a first LPM or CPM were included. The study included 40 828 patients with CPM and 1487 with LPM. After propensity score matching 1344 patients with CPM were matched 1:1 with patients treated with LPM. Patients with LPM had a lower rate of all-cause and cardiovascular death within the 30 days after implantation. During subsequent follow-up (mean: 8.6±10.5 months), risk of all-cause death in the unmatched population was significantly higher in the LPM group than in the CPM group, whereas risk of cardiovascular death and of endocarditis was not significantly different. After matching on all baseline characteristics including comorbidities (mean follow-up 6.2±8.7 months), all-cause death, cardiovascular death, and infective endocarditis were not statistically different in the 2 groups. Conclusions Patients treated with leadless VVI pacemakers had better clinical outcomes in the first month compared with the patients treated with conventional VVI pacing. During a midterm follow-up, risk of all-cause death, cardiovascular death, and endocarditis in patients treated with leadless VVI pacemaker was not statistically different after propensity score matching.
背景 无导线心室永久起搏器(无导线 VVI 或 LPM)旨在降低传统 VVI 起搏器(CPM)相关的导线并发症。我们的研究旨在评估和比较两种技术在 30 天内和中期随访期间的真实临床结局。
方法和结果 这项法国纵向队列研究基于国家住院数据库。所有在 2017 年 1 月 1 日至 2020 年 9 月 1 日期间在法国医院住院的成年人(年龄≥18 岁),接受了首次 LPM 或 CPM 治疗的患者均被纳入研究。研究包括 40828 例 CPM 患者和 1487 例 LPM 患者。在进行倾向评分匹配后,将 1344 例 CPM 患者与 LPM 治疗的患者进行 1:1 匹配。在植入后的 30 天内,LPM 组的全因和心血管死亡发生率较低。在随后的随访期间(平均:8.6±10.5 个月),未匹配人群中 LPM 组的全因死亡风险显著高于 CPM 组,而心血管死亡和心内膜炎的风险无显著差异。在匹配所有基线特征(包括合并症)后(平均随访 6.2±8.7 个月),两组的全因死亡、心血管死亡和感染性心内膜炎无统计学差异。
结论 与接受传统 VVI 起搏治疗的患者相比,接受无导线 VVI 起搏器治疗的患者在第一个月的临床结局更好。在中期随访中,经过倾向评分匹配后,接受无导线 VVI 起搏器治疗的患者的全因死亡、心血管死亡和心内膜炎风险无统计学差异。