Liang Jing-Bo, Yuan Hsiang-Yu, Li Kin-Kit, Wei Wan-In, Wong Samuel Yeung Shan, Tang Arthur, Riley Steven, Kwok Kin On
Department of Biomedical Sciences, Jockey Club College of Veterinary Medicine and Life Sciences, City University of Hong Kong, Hong Kong Special administrative regions, China.
Centre for Applied One Health Research and Policy Advice, City University of Hong Kong, Hong Kong Special administrative regions, China.
Comput Struct Biotechnol J. 2022;20:4052-4059. doi: 10.1016/j.csbj.2022.07.048. Epub 2022 Jul 30.
Two years into the coronavirus 2019 (COVID-19) pandemic, populations with less built-up immunity continued to devise ways to optimize social distancing measures (SDMs) relaxation levels for outbreaks triggered by SARS-CoV-2 and its variants to resume minimal economics activities while avoiding hospital system collapse.
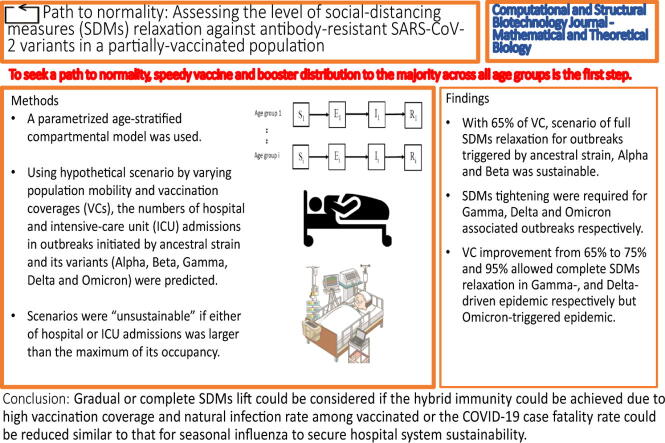
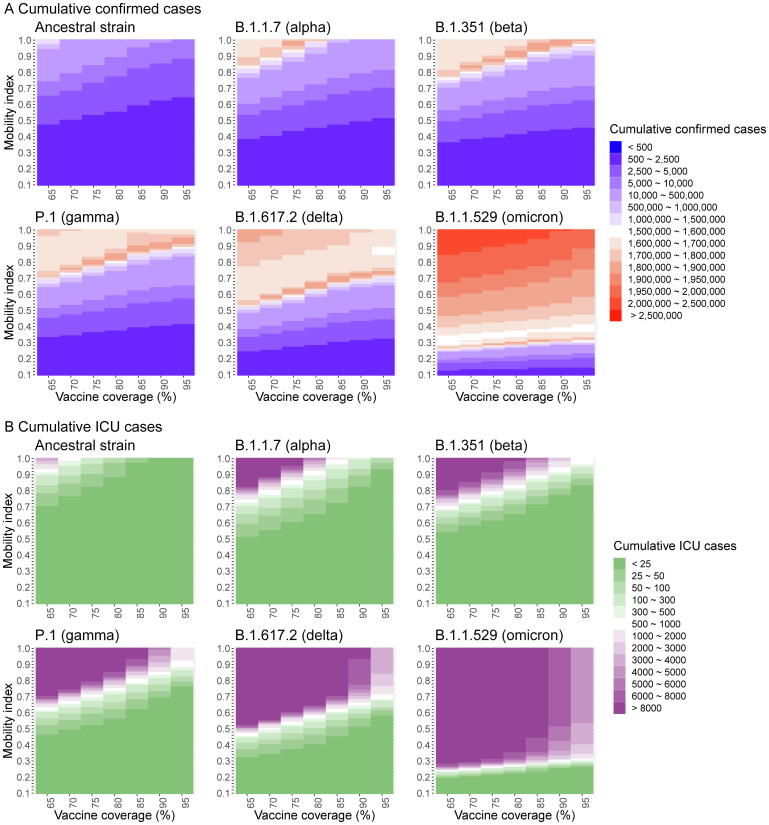
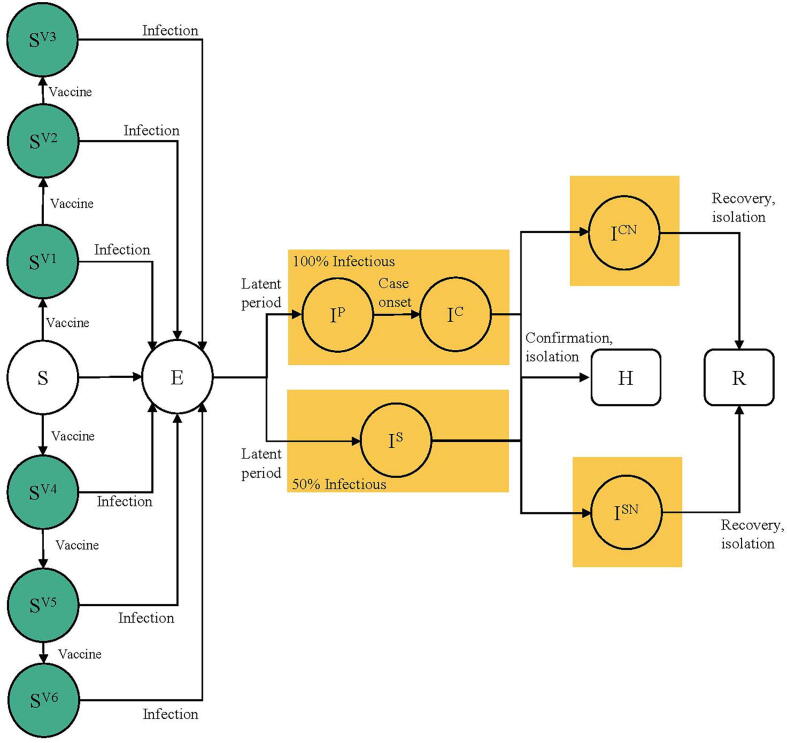
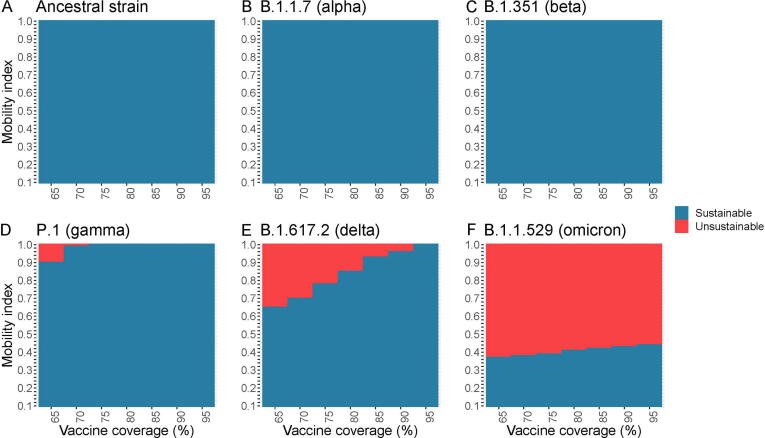
An age-stratified compartmental model featuring social mixing patterns was first fitted the incidence data in second wave in Hong Kong. Hypothetical scenario analysis was conducted by varying population mobility and vaccination coverages (VCs) to predict the number of hospital and intensive-care unit admissions in outbreaks initiated by ancestral strain and its variants (Alpha, Beta, Gamma, Delta and Omicron). Scenarios were "unsustainable" if either of admissions was larger than the maximum of its occupancy.
At VC of 65%, scenarios of full SDMs relaxation (mean daily social encounters prior to COVID-19 pandemic = 14.1 contacts) for outbreaks triggered by ancestral strain, Alpha and Beta were sustainable. Restricting levels of SDMs was required such that the optimal population mobility had to be reduced to 0.9, 0.65 and 0.37 for Gamma, Delta and Omicron associated outbreaks respectively. VC improvement from 65% to 75% and 95% allowed complete SDMs relaxation in Gamma-, and Delta-driven epidemic respectively. However, this was not supported for Omicron-triggered epidemic.
To seek a path to normality, speedy vaccine and booster distribution to the majority across all age groups is the first step. Gradual or complete SDMs lift could be considered if the hybrid immunity could be achieved due to high vaccination coverage and natural infection rate among vaccinated or the COVID-19 case fatality rate could be reduced similar to that for seasonal influenza to secure hospital system sustainability.
在2019冠状病毒病(COVID-19)大流行的两年中,人群中已建立的免疫力较低,他们继续设法优化社交距离措施(SDM)的放松程度,以应对由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)及其变体引发的疫情,从而在避免医院系统崩溃的同时恢复最低限度的经济活动。
首先将一个具有社会混合模式的年龄分层隔间模型拟合到香港第二波疫情的发病率数据中。通过改变人群流动性和疫苗接种覆盖率(VC)进行假设情景分析,以预测由原始毒株及其变体(阿尔法、贝塔、伽马、德尔塔和奥密克戎)引发的疫情中医院和重症监护病房的入院人数。如果任何一种入院人数超过其最大容量,则这些情景为“不可持续”。
在疫苗接种覆盖率为65%时,由原始毒株、阿尔法和贝塔引发的疫情中,完全放松社交距离措施的情景(COVID-19大流行前平均每日社交接触次数=14.1次)是可持续的。对于与伽马、德尔塔和奥密克戎相关的疫情,需要限制社交距离措施的水平,使得最佳人群流动性分别降至0.9、0.65和0.37。疫苗接种覆盖率从65%提高到75%和95%分别允许在伽马和德尔塔驱动的疫情中完全放松社交距离措施。然而,对于奥密克戎引发的疫情则不支持这样做。
为了寻求恢复正常的途径,第一步是迅速为所有年龄组的大多数人分发疫苗和加强针。如果由于高疫苗接种覆盖率和接种者中的自然感染率而实现了混合免疫,或者COVID-19病死率可以降低到与季节性流感相似的水平以确保医院系统的可持续性,则可以考虑逐步或完全取消社交距离措施。