Jockey Club School of Public Health and Primary Care, Chinese University of Hong Kong, Hong Kong Special Administrative Region, China; Li Ka Shing Institute of Health Sciences, Faculty of Medicine, Chinese University of Hong Kong, Hong Kong Special Administrative Region, China.
Department of Medicine and Therapeutics, Chinese University of Hong Kong, Hong Kong Special Administrative Region, China.
Lancet Microbe. 2023 Jun;4(6):e418-e430. doi: 10.1016/S2666-5247(23)00006-X. Epub 2023 Apr 20.
The primary aim of using vaccines in public health responses to SARS-CoV-2 variants of concern is to reduce incidence of severe disease, for which T-cell responses are essential. There is a paucity of data on vaccine-induced T-cell immunity to omicron (B.1.1.529). We aimed to compare SARS-CoV-2 omicron BA.1-specific T-cell responses in adults vaccinated with CoronaVac or BNT162b2.
For this observational cohort, we recruited adults (aged ≥18 years) from three vaccination centres in Hong Kong. We included participants from four cohorts (cohort 1: participants who received two doses of either BNT162b2 or CoronaVac, cohort 2: participants who received two doses and a booster, cohort 3: participants who received two doses and a booster and had a breakthrough omicron infection, and cohort 4: participants who had a previous non-omicron infection and subsequently received one dose of vaccine). People with confirmed history of COVID-19 at recruitment were excluded from cohort 1 and cohort 2. We collected blood samples before vaccination (for cohort 1 and 2), 1-month following vaccination (for all cohorts), and during convalescence for cohort 3 and 4) and determined the proportion of IFNγCD4 and IFNγCD8 T cells in peripheral blood against SARS-CoV-2 using flow cytometry with peptide pools of SARS-CoV-2 wild type or omicron BA.1. The primary outcome was proportion of CD4 and CD8 T cells against SARS-CoV-2 1 month after exposure (ie, vaccination or breakthrough infection).
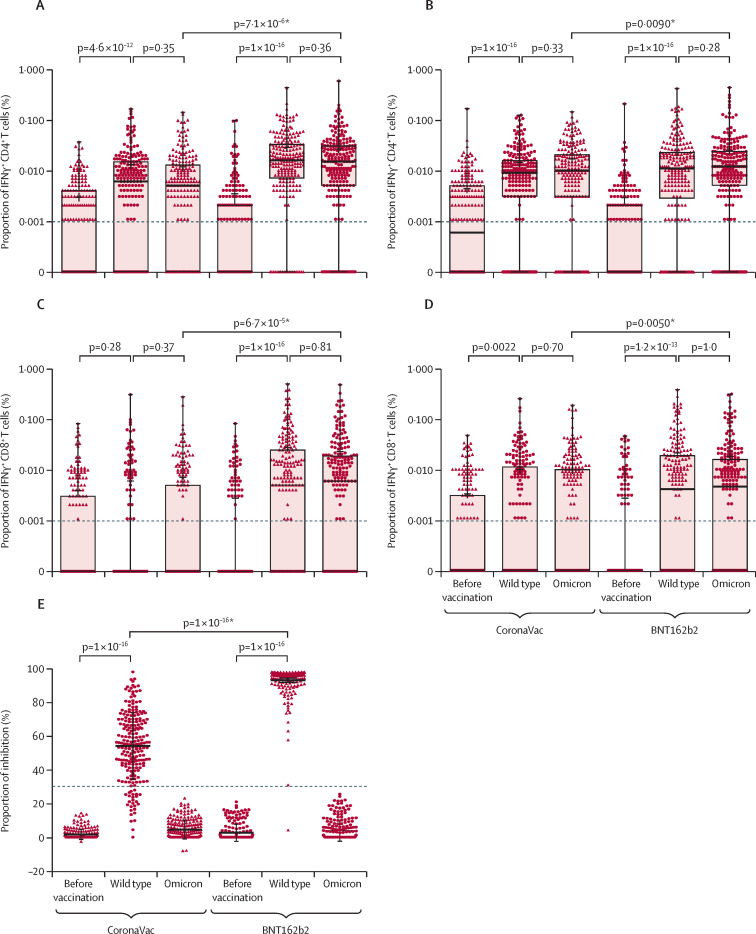
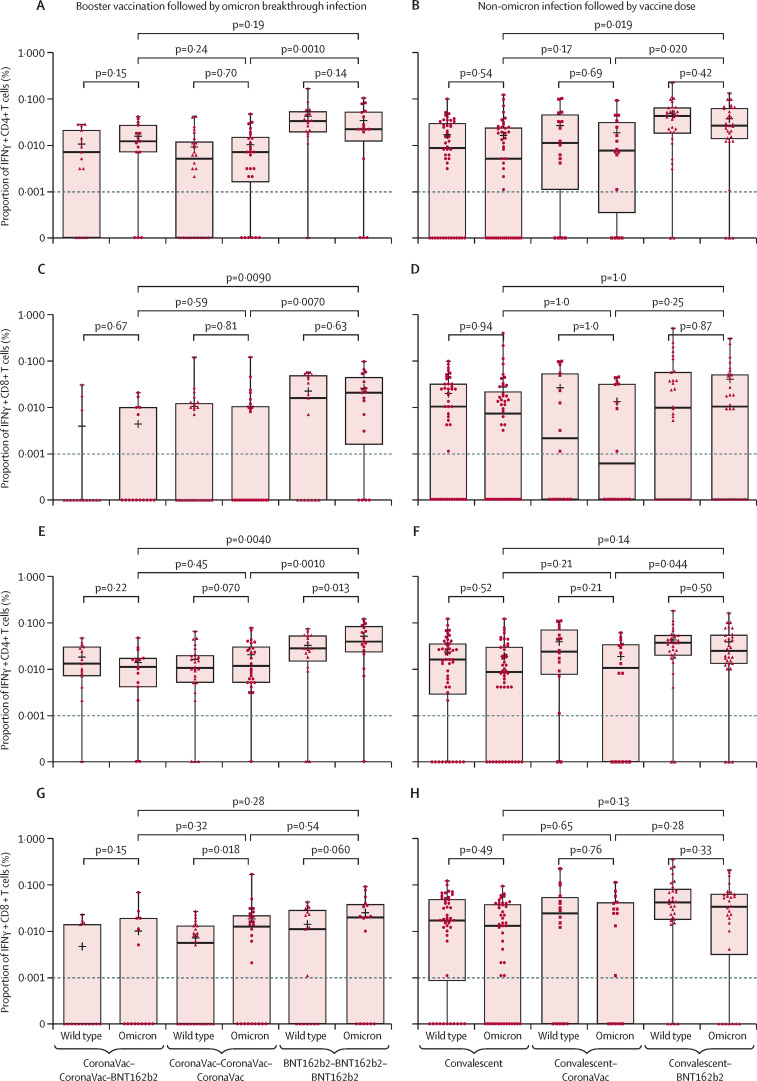
Overall, between May 21, 2020, and Aug 31, 2021, we recruited 659 participants (231 [35%] men and 428 [65%] women). Of these participants, 428 were included in cohort 1 (214 [50%] received BNT162b2 and 214 [50%] received CoronaVac); 127 in cohort 2 (48 [38%] received all BNT162b2, 40 [31%] received all CoronaVac, and 39 [31%] received two CoronaVac and a booster with BNT162b2); 58 in cohort 3, and 46 in cohort 4 (16 [35%] received CoronaVac and 30 [65%] received BNT162b2). Vaccine-induced T-cell responses to the wild-type and omicron BA.1 variants were generally similar in adults receiving two doses of either CoronaVac (CD4 cells p=0·33; CD8 cells p=0·70) or BNT162b2 (CD4 cells p=0·28; CD8 cells p=1·0). Using a peptide pool of all structural proteins for stimulation, BNT162b2 induced a higher median frequency of omicron-specific CD4 T cells in adults younger than 60 years (CD4 cells 0·012% vs 0·010%, p=0·031; CD8 cells 0·003% vs 0·000%, p=0·055) and omicron-specific CD8 T cells in people aged 60 years or older (CD4 cells 0·015% vs 0·006%, p=0·0070; CD8 cells 0·007% vs 0·000%, p=0·035). A booster dose of either BNT162b2 or CoronaVac after two doses of CoronaVac boosted waning T-cell responses, but T-cell responses did not exceed those at 1 month after the second dose (CoronaVac CD4 p=0·41, CD8 p=0·79; BNT162b2 CD4 p=0·70 CD8 p=0·80).
The evidence that mRNA and inactivated vaccines based on the ancestral SARS-CoV-2 virus elicited T-cell responses to SARS-CoV-2 omicron variants might explain the high observed vaccine effectiveness against severe COVID-19 shown by both types of vaccine, despite great differences in neutralising antibody responses. The use of either vaccine can be considered if the primary aim is to reduce severity and death caused by the new omicron subvariants; however, BNT162b2 is preferable for adults older than 60 years.
The Health and Medical Research Fund Commissioned Research on the Novel Coronavirus Disease and S H Ho Foundation.
在针对 SARS-CoV-2 变体的公共卫生应对中使用疫苗的主要目的是降低严重疾病的发生率,而 T 细胞反应是必不可少的。关于针对 omicron(B.1.1.529)的疫苗诱导 T 细胞免疫的数据很少。我们旨在比较接种 CoronaVac 或 BNT162b2 的成年人中针对 SARS-CoV-2 omicron BA.1 的特异性 T 细胞反应。
对于这项观察性队列研究,我们从香港的三个疫苗接种中心招募了成年人(年龄≥18 岁)。我们纳入了四个队列的参与者(队列 1:接受两剂 BNT162b2 或 CoronaVac 的参与者;队列 2:接受两剂和加强针的参与者;队列 3:接受两剂和加强针且发生突破性 omicron 感染的参与者;队列 4:有既往非 omicron 感染史且随后接种一剂疫苗的参与者)。从招募时起就已确认有 COVID-19 病史的人被排除在队列 1 和队列 2 之外。我们在接种前(队列 1 和 2)、接种后 1 个月(所有队列)以及队列 3 和 4 的恢复期收集血液样本,并使用 SARS-CoV-2 野生型或 omicron BA.1 的肽池通过流式细胞术确定外周血中针对 SARS-CoV-2 的 IFNγCD4 和 IFNγCD8 T 细胞的比例。主要结局是接触(即接种或突破性感染)后 1 个月时针对 SARS-CoV-2 的 CD4 和 CD8 T 细胞的比例。
总体而言,在 2020 年 5 月 21 日至 2021 年 8 月 31 日期间,我们招募了 659 名参与者(231 名[35%]男性和 428 名[65%]女性)。其中,428 名参与者被纳入队列 1(214 名[50%]接受 BNT162b2,214 名[50%]接受 CoronaVac);127 名参与者被纳入队列 2(48 名[38%]接受所有 BNT162b2,40 名[31%]接受所有 CoronaVac,39 名[31%]接受两剂 CoronaVac 和一剂 BNT162b2 加强针);58 名参与者被纳入队列 3,46 名参与者被纳入队列 4(16 名[35%]接受 CoronaVac,30 名[65%]接受 BNT162b2)。在接受两剂 CoronaVac(CD4 细胞 p=0·33;CD8 细胞 p=0·70)或 BNT162b2(CD4 细胞 p=0·28;CD8 细胞 p=1·0)的成年人中,疫苗诱导针对野生型和 omicron BA.1 变体的 T 细胞反应通常相似。使用所有结构蛋白的肽池进行刺激时,BNT162b2 在年龄小于 60 岁的成年人中诱导更高的 omicron 特异性 CD4 T 细胞频率(CD4 细胞 0·012% vs 0·010%,p=0·031;CD8 细胞 0·003% vs 0·000%,p=0·055)和年龄在 60 岁或以上的成年人中诱导更高的 omicron 特异性 CD8 T 细胞频率(CD4 细胞 0·015% vs 0·006%,p=0·0070;CD8 细胞 0·007% vs 0·000%,p=0·035)。在接种两剂 CoronaVac 后接种一剂 BNT162b2 或 CoronaVac 的加强针增强了逐渐减弱的 T 细胞反应,但 T 细胞反应并未超过第二次接种后 1 个月的水平(CoronaVac CD4 p=0·41,CD8 p=0·79;BNT162b2 CD4 p=0·70,CD8 p=0·80)。
基于 SARS-CoV-2 原始病毒的 mRNA 和灭活疫苗诱导针对 SARS-CoV-2 omicron 变体的 T 细胞反应的证据可能解释了这两种类型的疫苗都显示出针对新的 omicron 亚变体的高观察到的疫苗有效性,尽管中和抗体反应存在很大差异。如果主要目的是降低新的 omicron 亚变体引起的严重疾病和死亡的发生率,可以考虑使用任何一种疫苗;然而,对于 60 岁以上的成年人,BNT162b2 是更好的选择。
卫生和医学研究基金委员会对新型冠状病毒疾病的委托研究以及 S H Ho 基金会。