Mansour Mahmoud M, Fard Darian, Basida Sanket D, Obeidat Adham E, Darweesh Mohammad, Mahfouz Ratib, Ahmad Ali
Internal Medicine, University of Missouri School of Medicine, Columbia, USA.
Internal Medicine, University of Hawaii, Honolulu, USA.
Cureus. 2022 Jul 5;14(7):e26567. doi: 10.7759/cureus.26567. eCollection 2022 Jul.
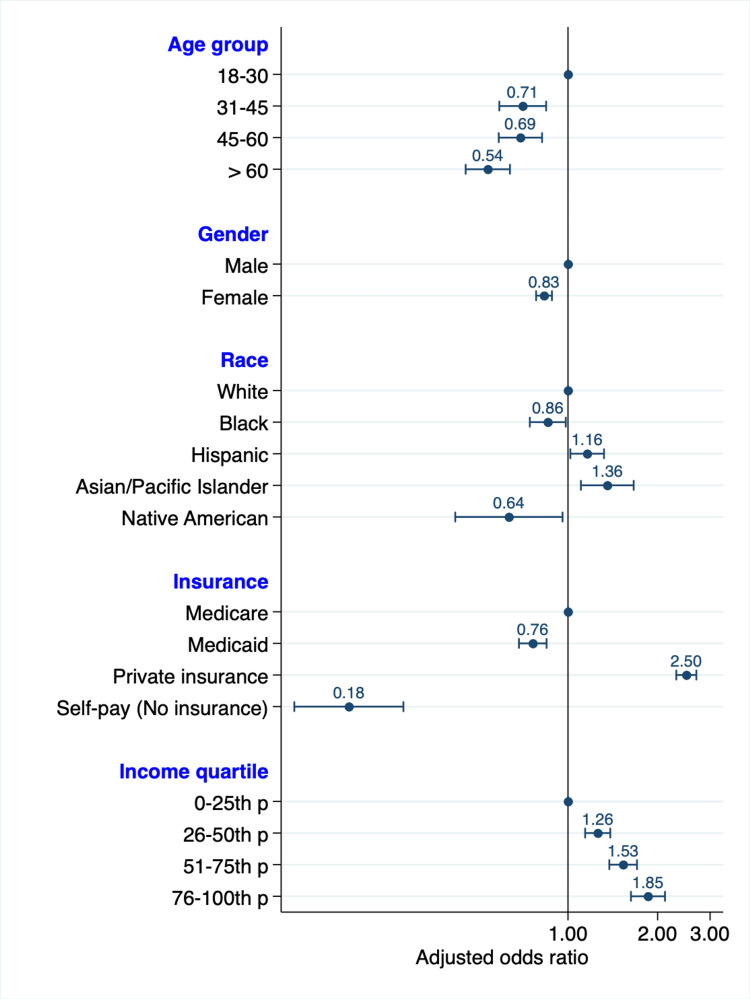
Background Liver transplantation is the life-saving standard of care for those with end-stage liver disease. Unfortunately, many patients on the liver transplant list die waiting. Several studies have demonstrated significant differences based on disparities in race, gender, and multiple socioeconomic factors. We sought to evaluate recent disparities among patients receiving liver transplants using the latest available data from the National Inpatient Sample (NIS), the largest publicly available inpatient care database in the United States. Methods We performed an analysis of discharge data from the NIS between 2016 and 2019. We identified adult patients with chronic liver disease who underwent a liver transplant using the International Classification of Diseases, 10th revision (ICD-10) codes. Multivariate logistic regression was used to adjust for differences in race, gender, socioeconomic status, and comorbidities among those who received a liver transplant. Results A total of 24,595 liver transplants were performed over the study period. Female gender was independently associated with decreased transplant rates (adjusted odds ratio (AOR) 0.83, 95% confidence interval (CI), 0.78-0.89, P < 0.001). Compared to White patients, Black patients had decreased transplant rates (AOR 0.86, 95% CI, 0.75-0.99, P = 0.034), as did Native Americans (AOR 0.64; 95% CI, 0.42-0.97, P = 0.035). Hispanics and Asian Americans had increased rates of liver transplantation (AOR 1.16, 95% CI 1.02-1.32, P = 0.022, and 1.36, 95% CI 1.11-1.67, P = 0.003; respectively). The increase in income quartile was associated with an incremental increase in transplant rates. Additionally, patients with private insurance had much higher transplant rates compared to those with Medicare (AOR 2.50, 95% CI 2.31-2.70, P < 0.001) while patients without insurance had the lowest rates of transplantation (AOR 0.18, 95% CI 0.12-0.28, P < 0.001). Conclusions Our analysis demonstrates that race, gender, and other social determinants of health have significant impacts on the likelihood of receiving a liver transplant. Our study, on a national level, confirms previously described disparities in receiving liver transplantation. Patient-level studies are needed to better understand how these variables translate into differing liver transplantation rates.
背景 肝移植是终末期肝病患者的救命标准治疗方法。不幸的是,许多列入肝移植名单的患者在等待中死亡。多项研究表明,基于种族、性别和多种社会经济因素的差异存在显著不同。我们试图利用美国最大的公开可用住院护理数据库——国家住院样本(NIS)的最新数据,评估接受肝移植患者之间最近的差异。方法 我们对2016年至2019年NIS的出院数据进行了分析。我们使用国际疾病分类第十版(ICD - 10)编码确定了接受肝移植的成年慢性肝病患者。多因素逻辑回归用于调整接受肝移植者在种族、性别、社会经济地位和合并症方面的差异。结果 在研究期间共进行了24595例肝移植。女性与移植率降低独立相关(调整后的优势比[AOR]为0.83,95%置信区间[CI]为0.78 - 0.89,P < 0.001)。与白人患者相比,黑人患者的移植率降低(AOR为0.86,95%CI为0.75 - 0.99,P = 0.034),美国原住民也是如此(AOR为0.64;95%CI为0.42 - 0.97,P = 0.035)。西班牙裔和亚裔美国人的肝移植率有所增加(分别为AOR 1.16,95%CI 1.02 - 1.32,P = 0.022;以及AOR 1.36,95%CI 1.11 - 1.67,P = 0.003)。收入四分位数的增加与移植率的逐步上升相关。此外,与医疗保险患者相比,拥有私人保险的患者移植率要高得多(AOR 2.50,95%CI 2.31 - 2.70,P < 0.001),而无保险患者的移植率最低(AOR 0.18,95%CI 0.12 - 0.28,P < 0.001)。结论 我们的分析表明,种族、性别和其他健康社会决定因素对接受肝移植的可能性有重大影响。我们在全国范围内的研究证实了先前描述的肝移植差异。需要进行患者层面的研究,以更好地了解这些变量如何转化为不同的肝移植率。