Smeele Patrick J, Vermunt Lisa, Blok Siebe, Duitman Jan Willem, Nossent Esther J, van Agtmael Michiel A, Heunks Leo M A, Horn Janneke, Bogaard Harm Jan, Teunissen Charlotte E
Neurochemistry Laboratory, Department of Clinical Chemistry, Amsterdam Neuroscience, Vrije Universiteit Amsterdam, Amsterdam UMC, Amsterdam, the Netherlands.
Department of Pulmonary Medicine, Amsterdam University Medical Centre, Amsterdam 1081 HV, the Netherlands.
Brain Commun. 2022 Jul 26;4(4):fcac195. doi: 10.1093/braincomms/fcac195. eCollection 2022.
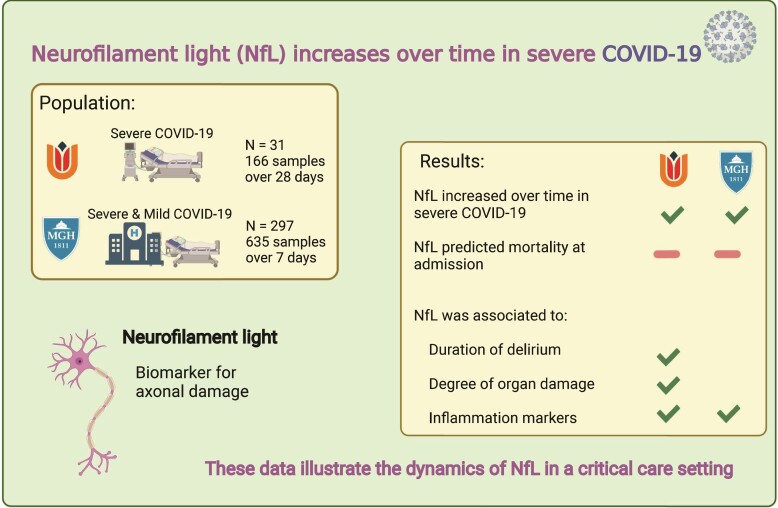
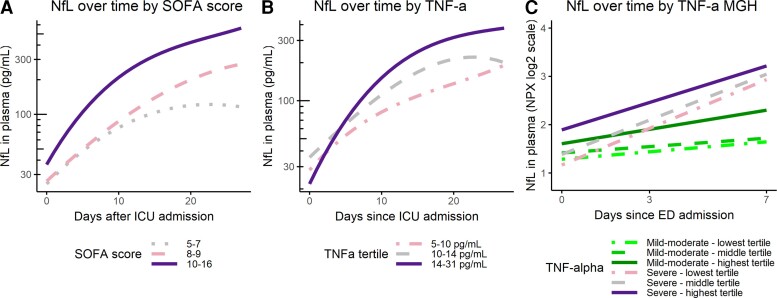
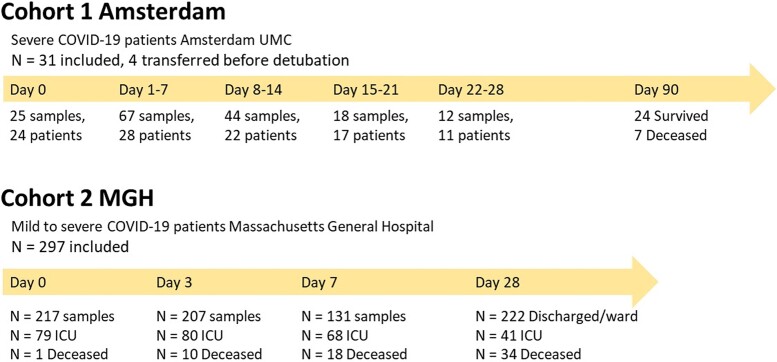
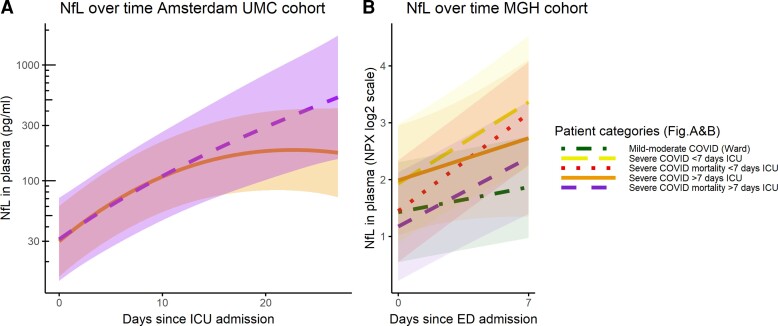
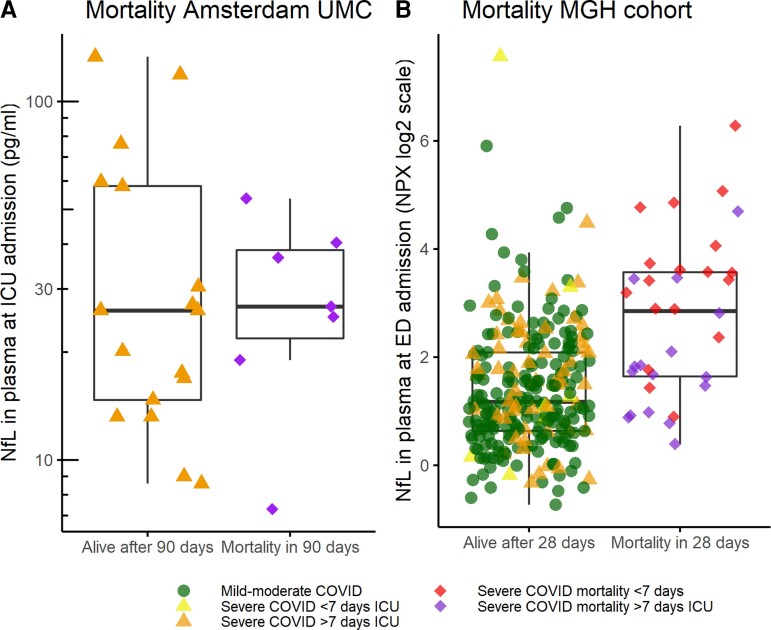
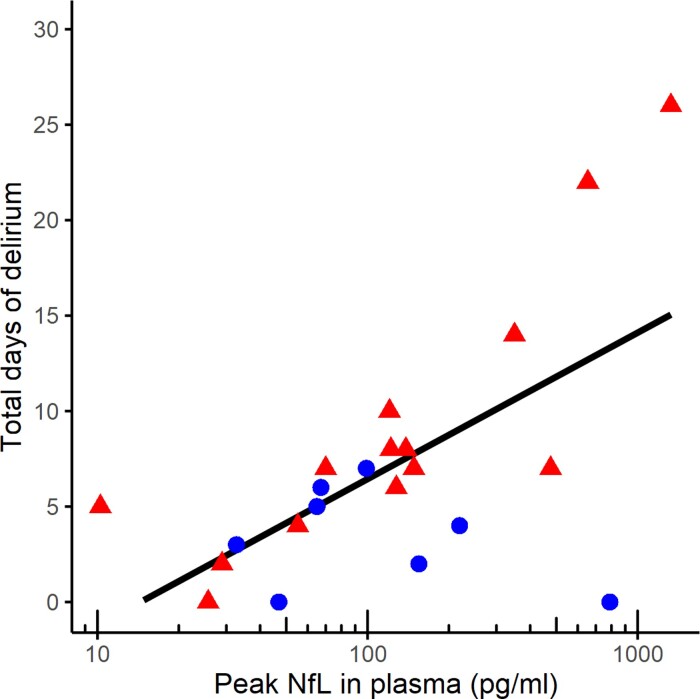
Neurological monitoring in sedated Intensive Care Unit patients is constrained by the lack of reliable blood-based biomarkers. Neurofilament light is a cross-disease biomarker for neuronal damage with potential clinical applicability for monitoring Intensive Care Unit patients. We studied the trajectory of neurofilament light over a month in Intensive Care Unit patients diagnosed with severe COVID-19 and explored its relation to clinical outcomes and pathophysiological predictors. Data were collected over a month in 31 Intensive Care Unit patients (166 plasma samples) diagnosed with severe COVID-19 at Amsterdam University Medical Centre, and in the first week after emergency department admission in 297 patients with COVID-19 (635 plasma samples) admitted to Massachusetts General hospital. We observed that Neurofilament light increased in a non-linear fashion in the first month of Intensive Care Unit admission and increases faster in the first week of Intensive Care Unit admission when compared with mild-moderate COVID-19 cases. We observed that baseline Neurofilament light did not predict mortality when corrected for age and renal function. Peak neurofilament light levels were associated with a longer duration of delirium after extubation in Intensive Care Unit patients. Disease severity, as measured by the sequential organ failure score, was associated to higher neurofilament light values, and tumour necrosis factor alpha levels at baseline were associated with higher levels of neurofilament light at baseline and a faster increase during admission. These data illustrate the dynamics of Neurofilament light in a critical care setting and show associations to delirium, disease severity and markers for inflammation. Our study contributes to determine the clinical utility and interpretation of neurofilament light levels in Intensive Care Unit patients.
在镇静的重症监护病房患者中,神经监测受到缺乏可靠血液生物标志物的限制。神经丝轻链是一种用于神经元损伤的跨疾病生物标志物,对监测重症监护病房患者具有潜在的临床适用性。我们研究了诊断为重症 COVID-19 的重症监护病房患者一个月内神经丝轻链的变化轨迹,并探讨了其与临床结局和病理生理预测指标的关系。在阿姆斯特丹大学医学中心,对 31 名诊断为重症 COVID-19 的重症监护病房患者(166 份血浆样本)进行了为期一个月的数据收集;在麻省总医院,对 297 名 COVID-19 患者(635 份血浆样本)在急诊科入院后的第一周进行了数据收集。我们观察到,在重症监护病房入院的第一个月,神经丝轻链呈非线性增加,与轻中度 COVID-19 病例相比,在重症监护病房入院的第一周增加更快。我们观察到,在校正年龄和肾功能后,基线神经丝轻链不能预测死亡率。重症监护病房患者拔管后,神经丝轻链峰值水平与谵妄持续时间延长有关。用序贯器官衰竭评分衡量的疾病严重程度与较高的神经丝轻链值相关,基线时肿瘤坏死因子α水平与基线时较高的神经丝轻链水平及入院期间更快的升高相关。这些数据说明了神经丝轻链在重症监护环境中的动态变化,并显示了其与谵妄、疾病严重程度和炎症标志物的关联。我们的研究有助于确定神经丝轻链水平在重症监护病房患者中的临床效用及解读。