Anesthesiology, Michigan Medicine, Ann Arbor, Michigan, USA.
New York Medical College, Valhalla, New York, USA.
BMJ Open. 2021 Sep 17;11(9):e050045. doi: 10.1136/bmjopen-2021-050045.
To characterise the clinical course of delirium for patients with COVID-19 in the intensive care unit, including postdischarge neuropsychological outcomes.
Retrospective chart review and prospective survey study.
Intensive care units, large academic tertiary-care centre (USA).
Patients (n=148) with COVID-19 admitted to an intensive care unit at Michigan Medicine between 1 March 2020 and 31 May 2020 were eligible for inclusion.
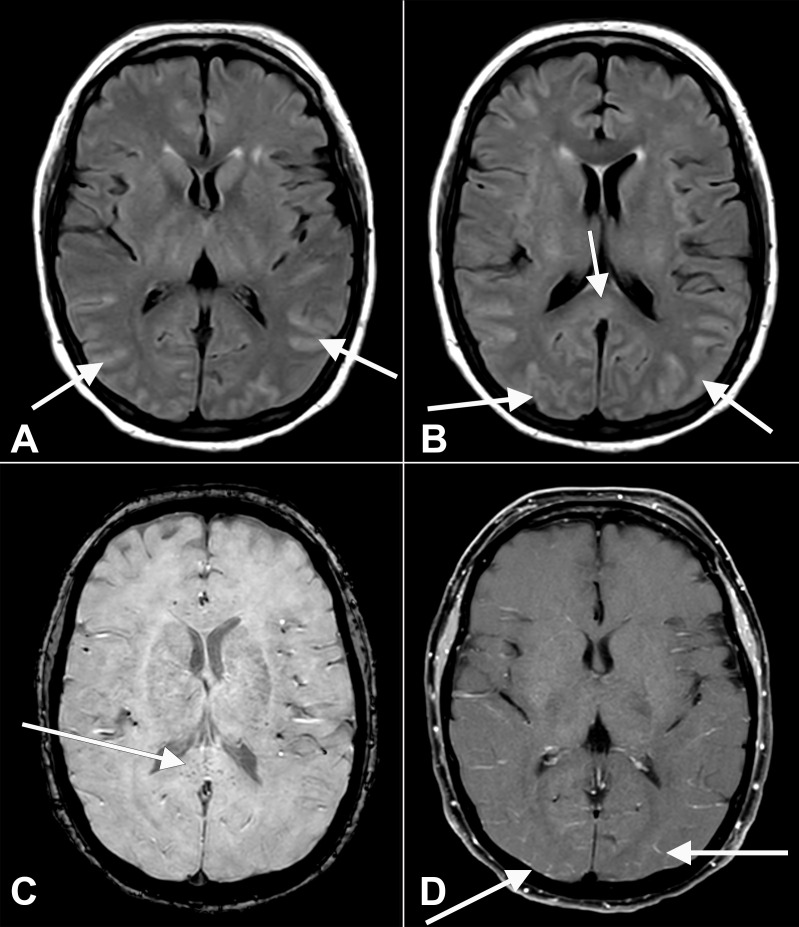
Delirium was the primary outcome, assessed via validated chart review method. Secondary outcomes included measures related to delirium, such as delirium duration, antipsychotic use, length of hospital and intensive care unit stay, inflammatory markers and final disposition. Neuroimaging data were also collected. Finally, a telephone survey was conducted between 1 and 2 months after discharge to determine neuropsychological function via the following tests: Family Confusion Assessment Method, Short Blessed Test, Patient-Reported Outcomes Measurement Information System Cognitive Abilities 4a and Patient-Health Questionnaire-9.
Delirium was identified in 108/148 (73%) patients, with median (IQR) duration lasting 10 (4-17) days. In the delirium cohort, 50% (54/108) of patients were African American and delirious patients were more likely to be female (76/108, 70%) (absolute standardised differences >0.30). Sedation regimens, inflammation, delirium prevention protocol deviations and hypoxic-ischaemic injury were likely contributing factors, and the most common disposition for delirious patients was a skilled care facility (41/108, 38%). Among patients who were delirious during hospitalisation, 4/17 (24%) later screened positive for delirium at home based on caretaker assessment, 5/22 (23%) demonstrated signs of questionable cognitive impairment or cognitive impairment consistent with dementia and 3/25 (12%) screened positive for depression within 2 months after discharge.
Patients with COVID-19 commonly experience a prolonged course of delirium in the intensive care unit, likely with multiple contributing factors. Furthermore, neuropsychological impairment may persist after discharge.
描述 COVID-19 患者在重症监护病房(ICU)的谵妄临床病程,包括出院后的神经心理学结局。
回顾性图表审查和前瞻性调查研究。
美国大型学术三级保健中心的 ICU。
2020 年 3 月 1 日至 5 月 31 日期间在密歇根大学医学中心 ICU 住院的 COVID-19 患者(n=148)符合入选条件。
谵妄是主要结局,通过验证的图表审查方法进行评估。次要结局包括与谵妄相关的指标,如谵妄持续时间、使用抗精神病药物、住院和 ICU 住院时间、炎症标志物和最终去向。还收集了神经影像学数据。最后,在出院后 1 至 2 个月进行电话调查,通过以下测试确定神经心理学功能:家庭谵妄评估方法、简短Blessed 测试、患者报告的结果测量信息系统认知能力 4a 和患者健康问卷-9。
148 例患者中有 108 例(73%)出现谵妄,中位(IQR)持续时间为 10(4-17)天。在谵妄组中,50%(54/108)的患者为非裔美国人,谵妄患者更可能为女性(76/108,70%)(绝对标准化差异>0.30)。镇静方案、炎症、谵妄预防方案偏差和缺氧缺血性损伤可能是促成因素,谵妄患者最常见的去向是熟练护理机构(41/108,38%)。在住院期间发生谵妄的患者中,根据照顾者评估,有 4/17(24%)人在出院后家中再次出现谵妄筛查阳性,5/22(23%)人出现可疑认知障碍或符合痴呆的认知障碍迹象,3/25(12%)人在出院后 2 个月内出现抑郁筛查阳性。
COVID-19 患者在 ICU 中经常经历长时间的谵妄,可能有多种促成因素。此外,出院后可能仍存在神经心理学损伤。