Department of Blood and Marrow Transplant and Cellular Immunotherapy, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL.
Department of Cancer Epidemiology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL.
Blood Adv. 2022 Dec 27;6(24):6109-6119. doi: 10.1182/bloodadvances.2022008320.
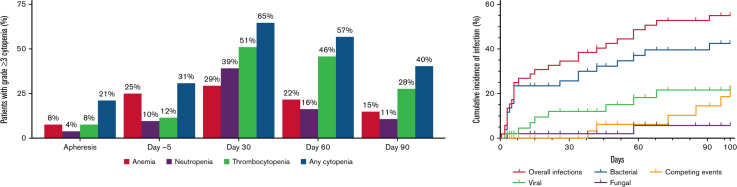
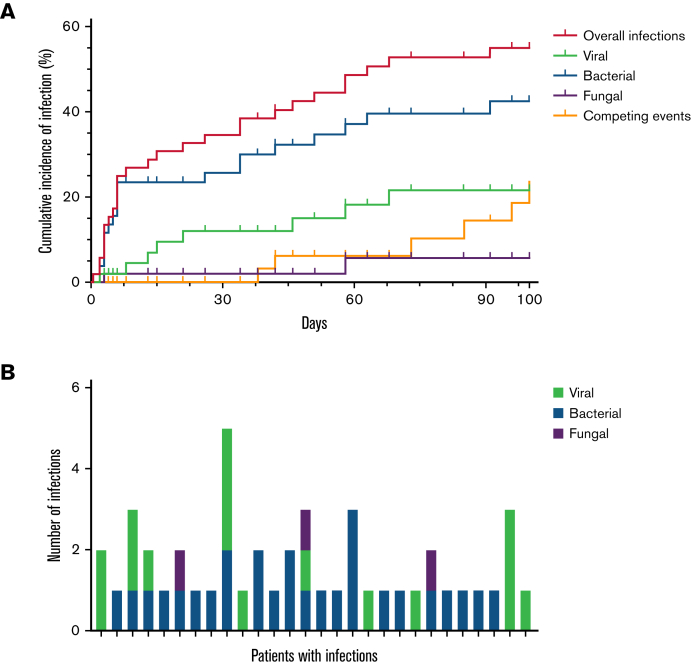
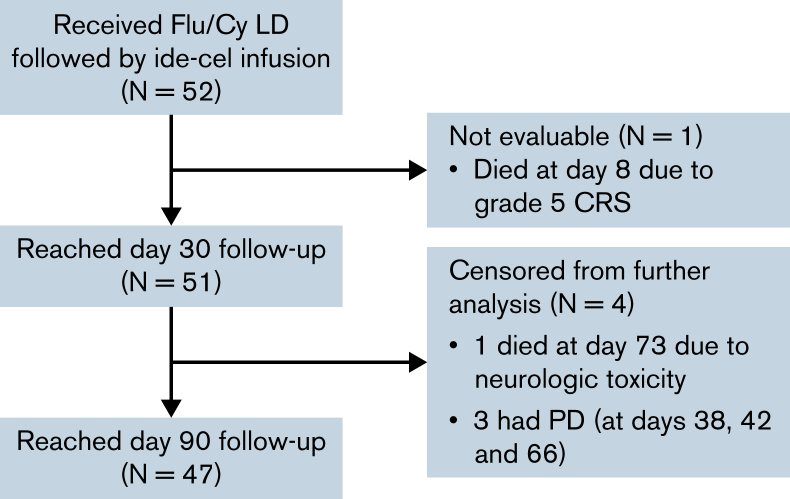
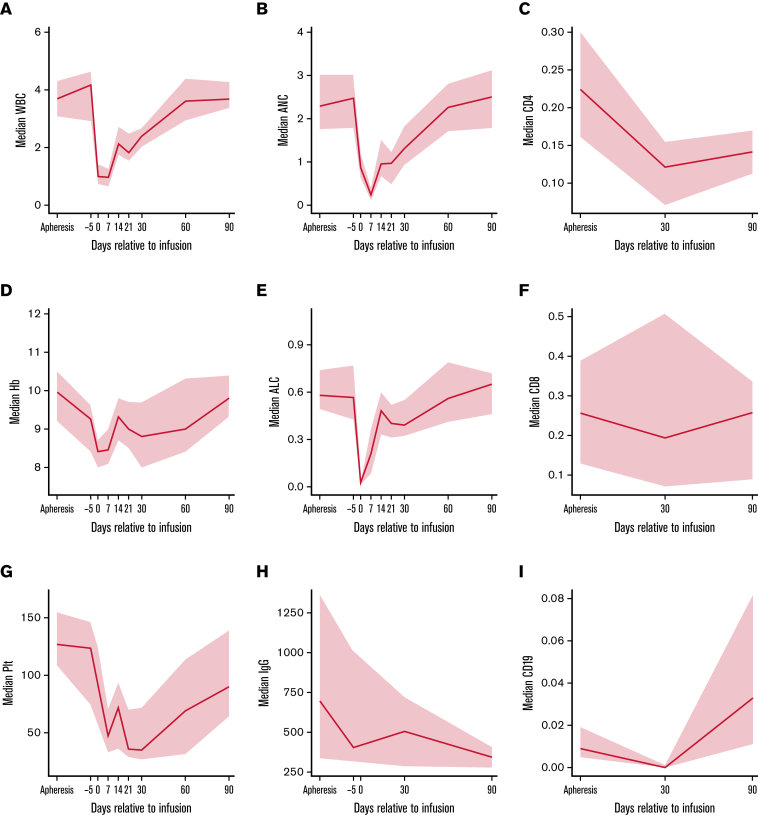
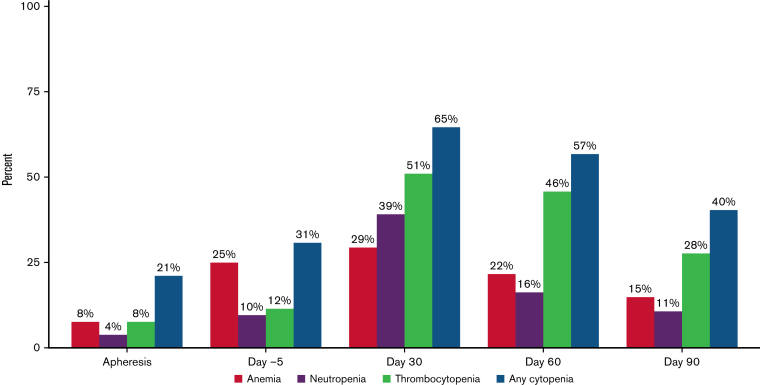
Idecabtagene vicleucel (ide-cel) was FDA-approved in March 2021 for the treatment of relapsed/refractory multiple myeloma after 4 lines of therapy. On the KarMMa trial, grade ≥ 3 cytopenias and infections were common. We sought to characterize cytopenias and infections within 100 days after ide-cel in the standard-of-care (SOC) setting. This multi-center retrospective study included 52 patients who received SOC ide-cel; 47 reached day-90 follow-up. Data were censored at day 100. Grade ≥ 3 cytopenia was present among 65% of patients at day 30 and 40% of patients at day 90. Granulocyte colony stimulating factor (G-CSF) was administered to 88%, packed red blood cell transfusions to 63%, platelet transfusions to 42%, thrombopoietin (TPO) agonists to 21%, intravenous immunoglobulin to 13%, and CD34+ stem cell boosts to 8%. At day 100, 19% and 13% of patients had ongoing use of TPO agonists and G-CSF, respectively. Infections occurred in 54% of patients and were grade ≥ 3 in 23%. Earlier infections in the first 30 days were typically bacterial (68%) and severe (50%). Later infections between days 31 and 100 were 50% bacterial and 42% viral; only 13% were grade ≥ 3. On univariate analysis, high pre-CAR-T marrow myeloma burden (≥ 50%), circulating plasma cells at pre-lymphodepletion (LD), and grade ≥ 3 anemia at pre-LD were associated with grade ≥ 3 cytopenia at both days 30 and 90. Longer time from last bridging treatment to LD was the only significant risk factor for infection.
伊达基仑(ide-cel)于 2021 年 3 月获得美国食品药品监督管理局(FDA)批准,用于治疗经过 4 线治疗后复发/难治性多发性骨髓瘤。在 KarMMa 试验中,≥3 级血液学毒性和感染较为常见。我们旨在描述 ide-cel 治疗后 100 天内血液学毒性和感染情况。这项多中心回顾性研究纳入了 52 例接受标准治疗(SOC)ide-cel 的患者;47 例患者达到了第 90 天随访。数据截止日期为第 100 天。第 30 天和第 90 天分别有 65%和 40%的患者出现≥3 级血液学毒性。88%的患者接受了粒细胞集落刺激因子(G-CSF)治疗,63%的患者接受了红细胞输注,42%的患者接受了血小板输注,21%的患者接受了血小板生成素(TPO)激动剂治疗,13%的患者接受了静脉注射免疫球蛋白治疗,8%的患者接受了 CD34+干细胞动员。第 100 天,分别有 19%和 13%的患者持续使用 TPO 激动剂和 G-CSF。54%的患者发生了感染,其中 23%为≥3 级感染。前 30 天发生的感染通常为细菌性(68%)和严重感染(50%)。第 31 天至第 100 天之间发生的感染为 50%细菌性和 42%病毒性;仅 13%为≥3 级感染。单因素分析显示,CAR-T 前骨髓中骨髓瘤负担较高(≥50%)、淋巴细胞耗竭前循环浆细胞(LD)、LD 前存在≥3 级贫血与第 30 天和第 90 天的≥3 级血液学毒性相关。从最后一次桥接治疗到 LD 的时间较长是感染的唯一显著危险因素。