Nakao Yosuke, Hayashi Hiromitsu, Yamashita Yo-Ichi, Takashi Ofuchi, Matsumura Kazuki, Uemura Norio, Kitamura Fumimasa, Itoyama Rumi, Yusa Toshihiko, Taki Katsunobu, Miyata Tatsunori, Higashi Takaaki, Nakagawa Shigeki, Okabe Hirohisa, Imai Katsunori, Baba Hideo
Department of Gastroenterological Surgery, Kumamoto University, Kumamoto 860-8556, Japan.
World J Clin Oncol. 2022 Jun 24;13(6):520-528. doi: 10.5306/wjco.v13.i6.520.
Although PNENs generally have a better prognosis than pancreatic cancers, some PNENs display malignant behavior including lymph node (LN) metastasis. Complete tumor resection can be the only potentially curative treatment for patients with resectable PNENs. However, the indications for LN dissection are still controversial. Over the last decade, minimally invasive surgery such as laparoscopic pancreatic surgery (LPS) has been increasingly performed for pancreatic tumors including PNENs.
To investigate the risk factors for LN metastasis in PNENs and to select appropriate patients for limited surgery by LPS.
From April 2001 to December 2019, 92 patients underwent pancreatic resection for PNENs at Kumamoto University Hospital. Finally, 82 patients were enrolled in this study. Using perioperative factors, we examined the predictive factors for LN metastasis in PNENs.
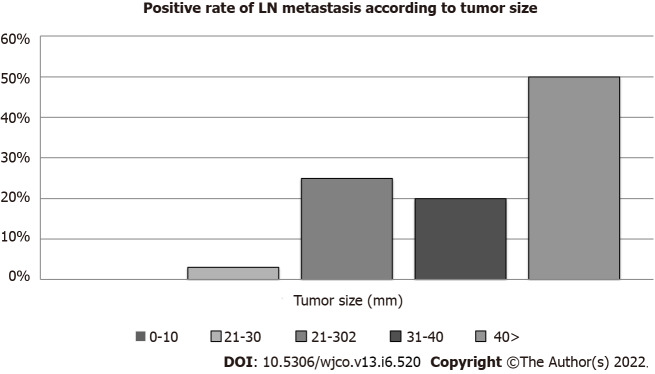
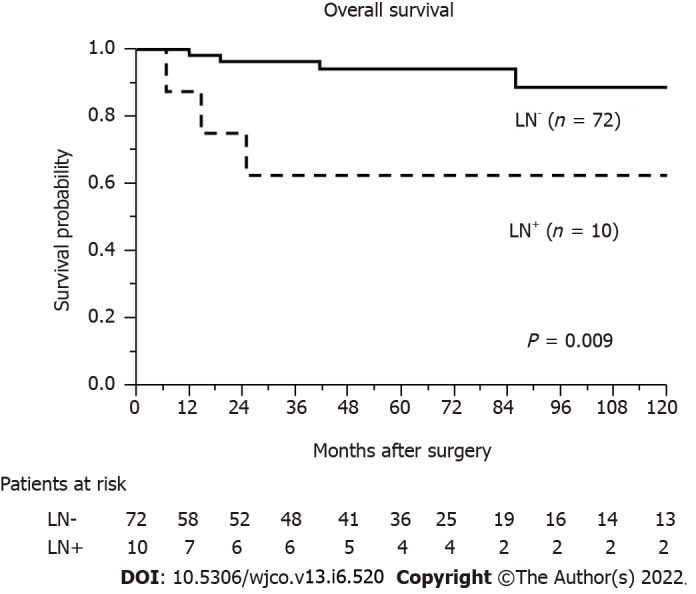
Among the 82 patients, the percentage of LN metastasis according to the pathological findings was 12% (10/82 cases). The median tumor size was 12 mm (range: 5-90 mm). The median tumor size in the LN-positive group (37 mm) was significantly larger than that in the LN-negative group (12 mm) ( = 0.0001). Multivariate analyses revealed that larger tumor size (≥ 20 mm) was an independent risk factor for LN metastasis (odds ratio 16.8, = 0.0062). In patients with small tumors (≤ 10 mm), LN metastasis was not found.
Larger tumor size (≥ 20 mm) is an independent risk factor for LN metastasis in PNENs. In smaller PNENs (≤ 10 mm), we may be able to choose limited surgery without LN dissection.
尽管胰腺神经内分泌肿瘤(PNENs)的预后通常比胰腺癌好,但一些PNENs表现出恶性行为,包括淋巴结(LN)转移。完整的肿瘤切除可能是可切除PNENs患者唯一潜在的治愈性治疗方法。然而,淋巴结清扫的指征仍存在争议。在过去十年中,诸如腹腔镜胰腺手术(LPS)等微创手术越来越多地用于包括PNENs在内的胰腺肿瘤。
探讨PNENs中淋巴结转移的危险因素,并选择合适的患者进行LPS有限手术。
2001年4月至2019年12月,92例患者在熊本大学医院接受了PNENs胰腺切除术。最终,82例患者纳入本研究。利用围手术期因素,我们研究了PNENs中淋巴结转移的预测因素。
82例患者中,根据病理结果,淋巴结转移率为12%(10/82例)。肿瘤大小中位数为12mm(范围:5 - 90mm)。淋巴结阳性组的肿瘤大小中位数(37mm)显著大于淋巴结阴性组(12mm)(P = 0.0001)。多因素分析显示,较大的肿瘤大小(≥20mm)是淋巴结转移的独立危险因素(比值比16.8,P = 0.0062)。在小肿瘤(≤10mm)患者中,未发现淋巴结转移。
较大的肿瘤大小(≥20mm)是PNENs中淋巴结转移的独立危险因素。对于较小的PNENs(≤10mm),我们或许能够选择不进行淋巴结清扫的有限手术。