Department of Respiratory Medicine, Tohoku University Hospital, Sendai, Japan.
Department of Biomedical Statistics and Bioinformatics, Kyoto University Graduate School of Medicine, Kyoto, Japan.
J Clin Oncol. 2022 Nov 1;40(31):3587-3592. doi: 10.1200/JCO.21.02911. Epub 2022 Aug 12.
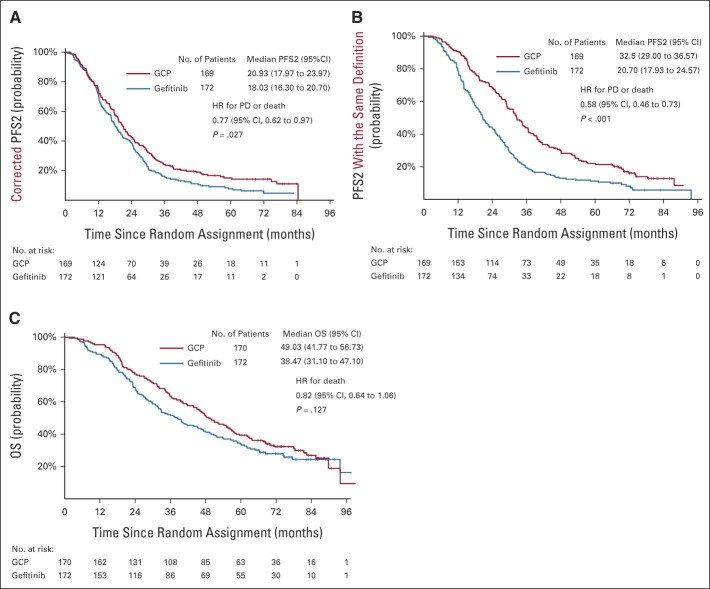
JCO In a randomized, open-label, phase III NEJ009 study, gefitinib plus chemotherapy significantly improved progression-free survival (PFS) and overall survival (OS) compared with gefitinib-alone in patients with untreated non-small-cell lung cancer harboring mutations in epidermal growth factor receptor. Herein, we report the updated survival outcome and long-term tolerability. Patients were randomly assigned to gefitinib (gefitinib 250 mg orally, once daily) and gefitinib combined with carboplatin plus pemetrexed (GCP in a 3-week cycle for six cycles followed by concurrent gefitinib and pemetrexed maintenance) groups. At the data cutoff (May 22, 2020), GCP demonstrated significantly better PFS2 (hazard ratio, 0.77; 95% CI, 0.62 to 0.97; = .027) than gefitinib. However, the updated median OS was 38.5 months (95% CI, 31.1 to 47.1) and 49.0 months (95% CI, 41.8 to 56.7) in the gefitinib and GCP groups, respectively (hazard ratio, 0.82; 95% CI, 0.64 to 1.06; = .127). The OS in both groups was similar for the overall patient population. No severe adverse events occurred since the first report. This updated analysis revealed that the GCP regimen improved PFS and PFS2 with an acceptable safety profile compared with gefitinib-alone. GCP is more efficient than gefitinib monotherapy as a first-line treatment for non-small-cell lung cancer with epidermal growth factor receptor mutations.
JCO 在一项随机、开放标签、III 期 NEJ009 研究中,与单独使用吉非替尼相比,吉非替尼联合化疗显著改善了未经治疗的表皮生长因子受体突变的非小细胞肺癌患者的无进展生存期(PFS)和总生存期(OS)。在此,我们报告了更新的生存结果和长期耐受性。患者被随机分配到吉非替尼(吉非替尼 250mg 口服,每日一次)和吉非替尼联合卡铂加培美曲塞(GCP,每 3 周为一周期,共 6 周期,随后同时给予吉非替尼和培美曲塞维持治疗)组。在数据截止日期(2020 年 5 月 22 日),GCP 显示出明显更好的 PFS2(风险比,0.77;95%CI,0.62 至 0.97;P=0.027)。然而,更新的中位 OS 分别为吉非替尼组 38.5 个月(95%CI,31.1 至 47.1)和 GCP 组 49.0 个月(95%CI,41.8 至 56.7)(风险比,0.82;95%CI,0.64 至 1.06;P=0.127)。对于总体患者人群,两组的 OS 相似。自首次报告以来,没有发生严重不良事件。这项更新的分析显示,与单独使用吉非替尼相比,GCP 方案改善了 PFS 和 PFS2,且具有可接受的安全性特征。GCP 作为表皮生长因子受体突变的非小细胞肺癌一线治疗药物,比吉非替尼单药更有效。