Department of Neurosurgery, Ludwig-Maximilians-University, Munich, Germany.
German Cancer Consortium (DKTK), Partner Site Munich, Munich, Germany.
Neuro Oncol. 2023 May 4;25(5):940-954. doi: 10.1093/neuonc/noac193.
Terminology to describe extent of resection in glioblastoma is inconsistent across clinical trials. A surgical classification system was previously proposed based upon residual contrast-enhancing (CE) tumor. We aimed to (1) explore the prognostic utility of the classification system and (2) define how much removed non-CE tumor translates into a survival benefit.
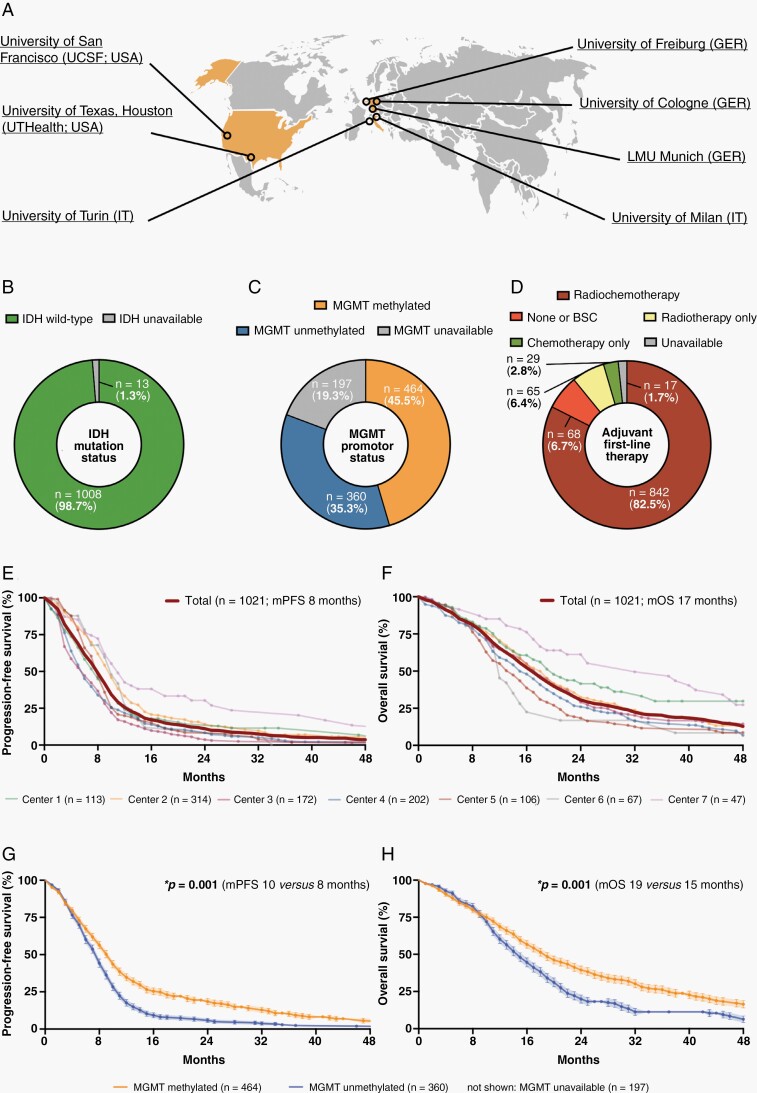
The international RANO resect group retrospectively searched previously compiled databases from 7 neuro-oncological centers in the USA and Europe for patients with newly diagnosed glioblastoma per WHO 2021 classification. Clinical and volumetric information from pre- and postoperative MRI were collected.
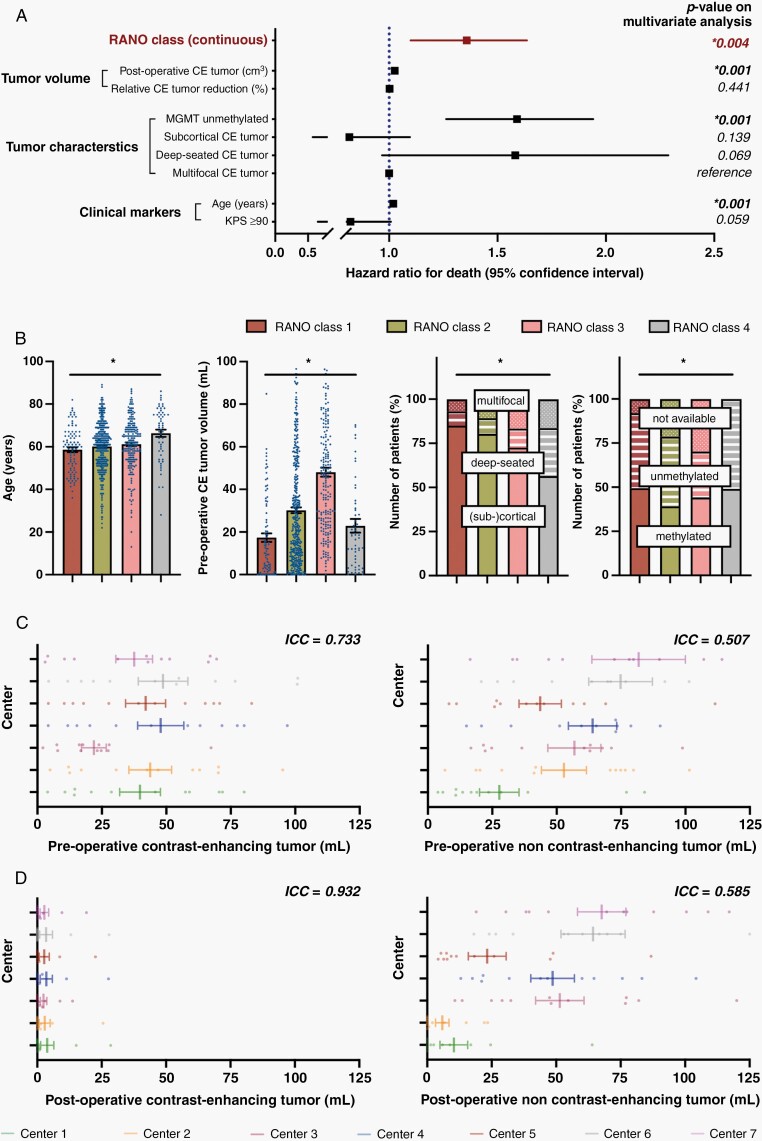
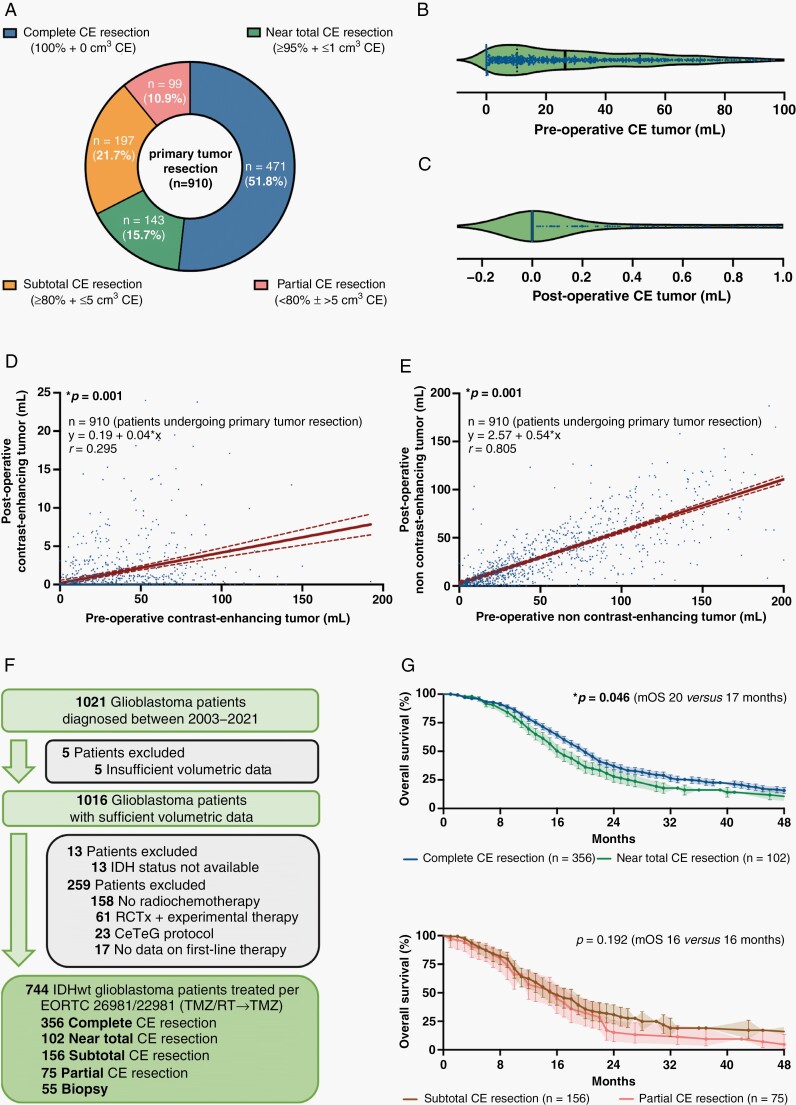
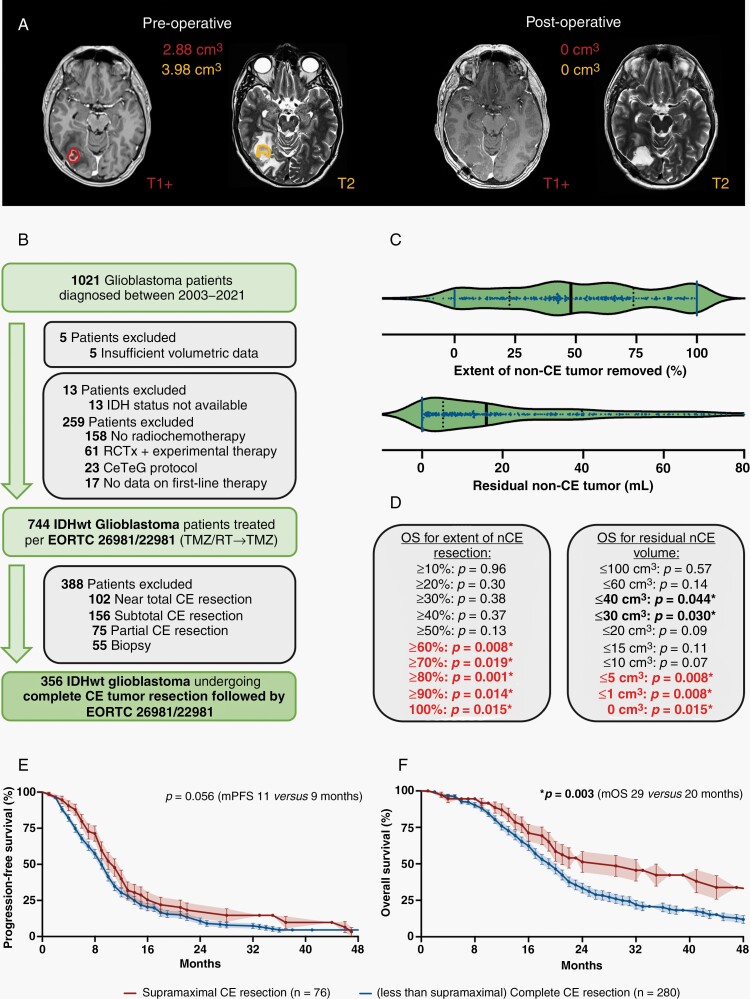
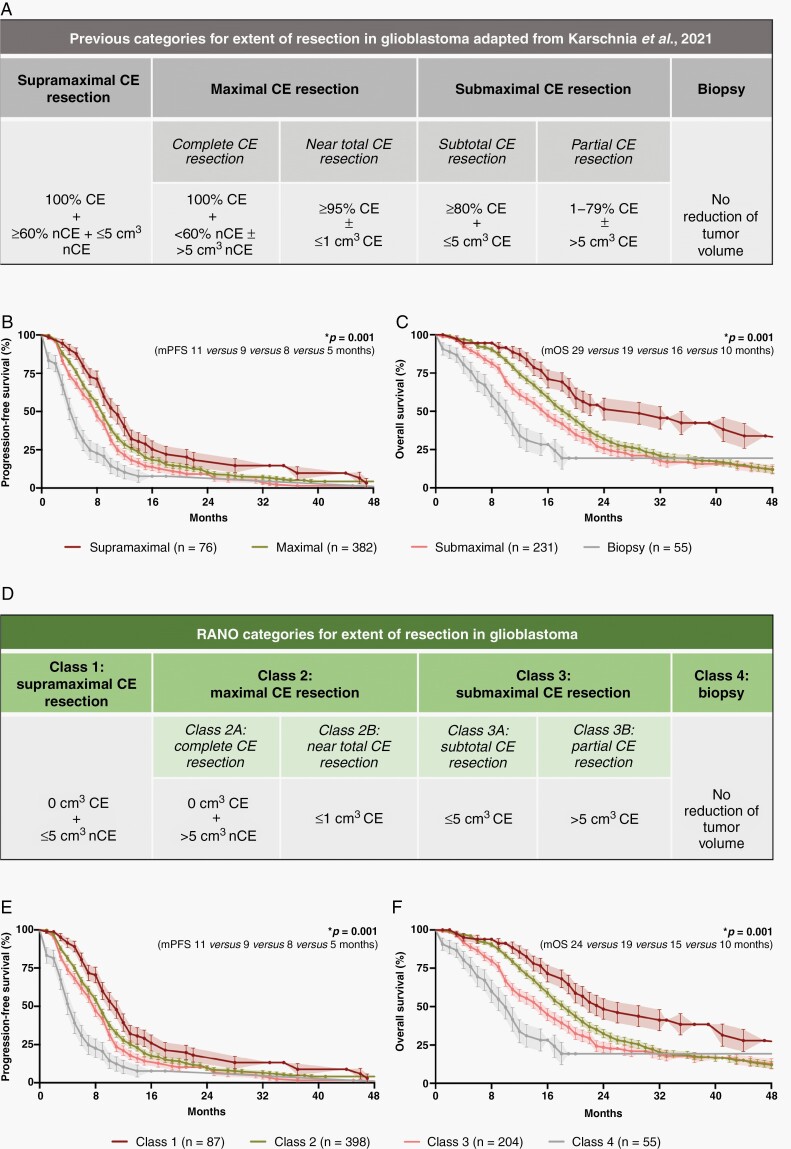
We collected 1,008 patients with newly diagnosed IDHwt glioblastoma. 744 IDHwt glioblastomas were treated with radiochemotherapy per EORTC-26981/22981 (TMZ/RT→TMZ) following surgery. Among these homogenously treated patients, lower absolute residual tumor volumes (in cm3) were favorably associated with outcome: patients with "maximal CE resection" (class 2) had superior outcome compared to patients with "submaximal CE resection" (class 3) or "biopsy" (class 4). Extensive resection of non-CE tumor (≤5 cm3 residual non-CE tumor) was associated with better survival among patients with complete CE resection, thus defining class 1 ("supramaximal CE resection"). The prognostic value of the resection classes was retained on multivariate analysis when adjusting for molecular and clinical markers.
The proposed "RANO categories for extent of resection in glioblastoma" are highly prognostic and may serve for stratification within clinical trials. Removal of non-CE tumor beyond the CE tumor borders may translate into additional survival benefit, providing a rationale to explicitly denominate such "supramaximal CE resection."
在胶质母细胞瘤的临床试验中,描述切除范围的术语不一致。之前提出了一种基于残留对比增强(CE)肿瘤的手术分类系统。我们旨在(1)探讨该分类系统的预后实用性,以及(2)定义切除多少非 CE 肿瘤可转化为生存获益。
国际 RANO 切除组回顾性地从美国和欧洲的 7 个神经肿瘤中心之前编译的数据库中搜索了根据 2021 年 WHO 分类新诊断的胶质母细胞瘤患者。收集了术前和术后 MRI 的临床和体积信息。
我们收集了 1008 例新诊断的 IDHwt 胶质母细胞瘤患者。744 例 IDHwt 胶质母细胞瘤在手术后接受了 EORTC-26981/22981(TMZ/RT→TMZ)放化疗。在这些同质治疗的患者中,较低的绝对残余肿瘤体积(cm3)与结果呈正相关:“最大 CE 切除”(2 类)患者的结果优于“次最大 CE 切除”(3 类)或“活检”(4 类)患者。在完全 CE 切除的患者中,广泛切除非 CE 肿瘤(残余非 CE 肿瘤≤5cm3)与更好的生存相关,从而定义为 1 类(“超最大 CE 切除”)。在调整分子和临床标志物后,多变量分析保留了切除等级的预后价值。
提出的“胶质母细胞瘤切除范围的 RANO 分类”具有高度的预后价值,可用于临床试验中的分层。切除 CE 肿瘤边界外的非 CE 肿瘤可能会带来额外的生存获益,为明确此类“超最大 CE 切除”提供了依据。