Brooke Hannah L, Mazzoni Anne-Sophie, Buffart Laurien M, Berntsen Sveinung, Nordin Karin, Demmelmaier Ingrid
Department of Surgical Sciences, Uppsala University, Uppsala, Sweden.
Department of Public Health and Caring Sciences, Uppsala University, Uppsala, Sweden.
BMC Sports Sci Med Rehabil. 2022 Aug 13;14(1):155. doi: 10.1186/s13102-022-00548-5.
Knowledge regarding adherence is necessary to improve the specificity of exercise interventions during cancer treatment. We aimed to determine adherence to resistance and endurance training interventions in parallel; identify subgroups with similar adherence characteristics; and examine determinants of these subgroups.
In the Phys-Can randomised controlled trial, participants (n = 577, 81% women, mean(SD) age 59(12) years, and 50% with BMI ≥ 25 kg/m) starting (neo-) adjuvant treatment for breast, colorectal or prostate cancer were randomized to 6-month of high (HI) or low-to-moderate intensity (LMI) supervised, group-based resistance training and individual home-based endurance training, with or without behavior change support. Adherence was calculated as performed exercise volume as a proportion of prescribed exercise volume (0-100%), overall (HI and LMI groups) and for frequency, intensity, type and time (FITT principles) (HI group). Adherence to resistance training was plotted against adherence to endurance training overall and for each FITT principle. K-means cluster analysis was used to identify subgroups with similar adherence characteristics. Potential determinants of subgroup membership were examined using multinomial logistic regression.
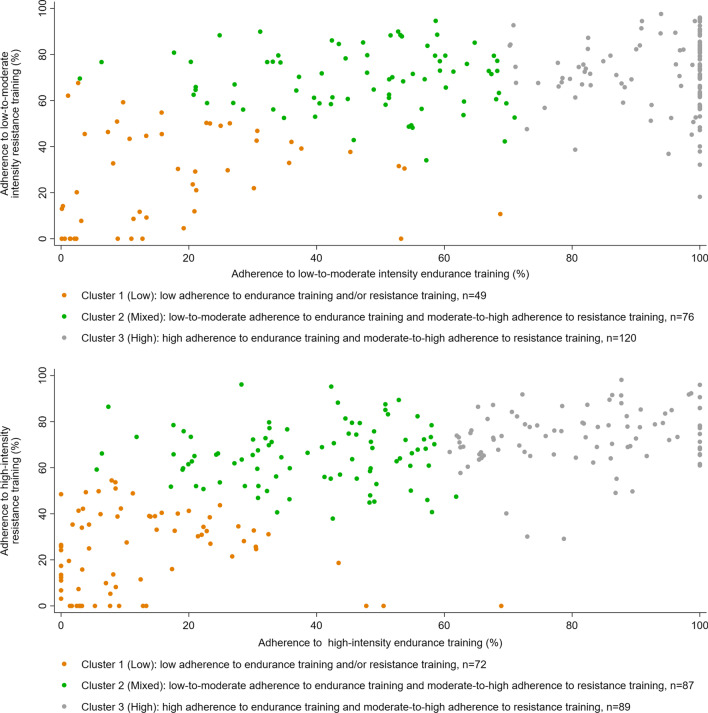
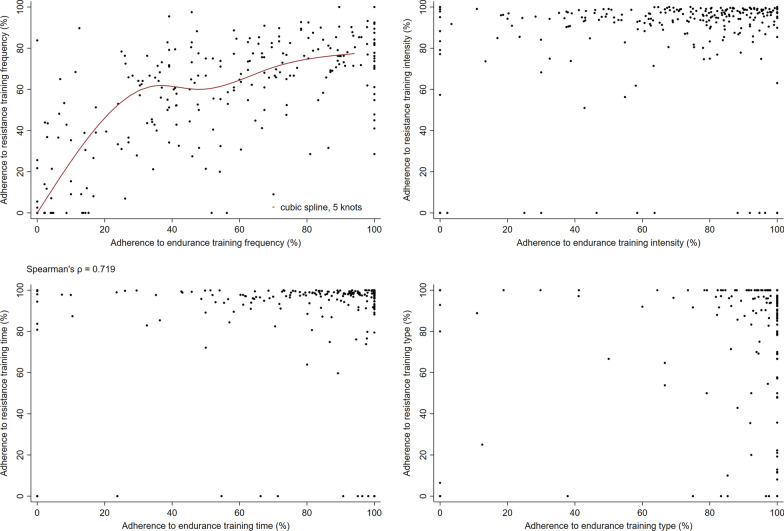
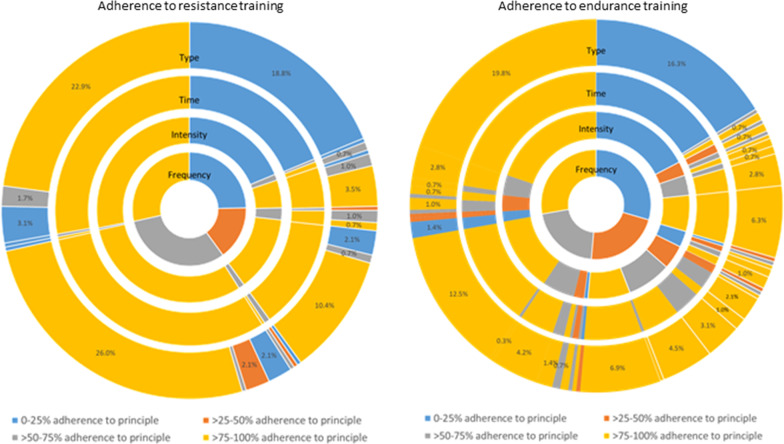
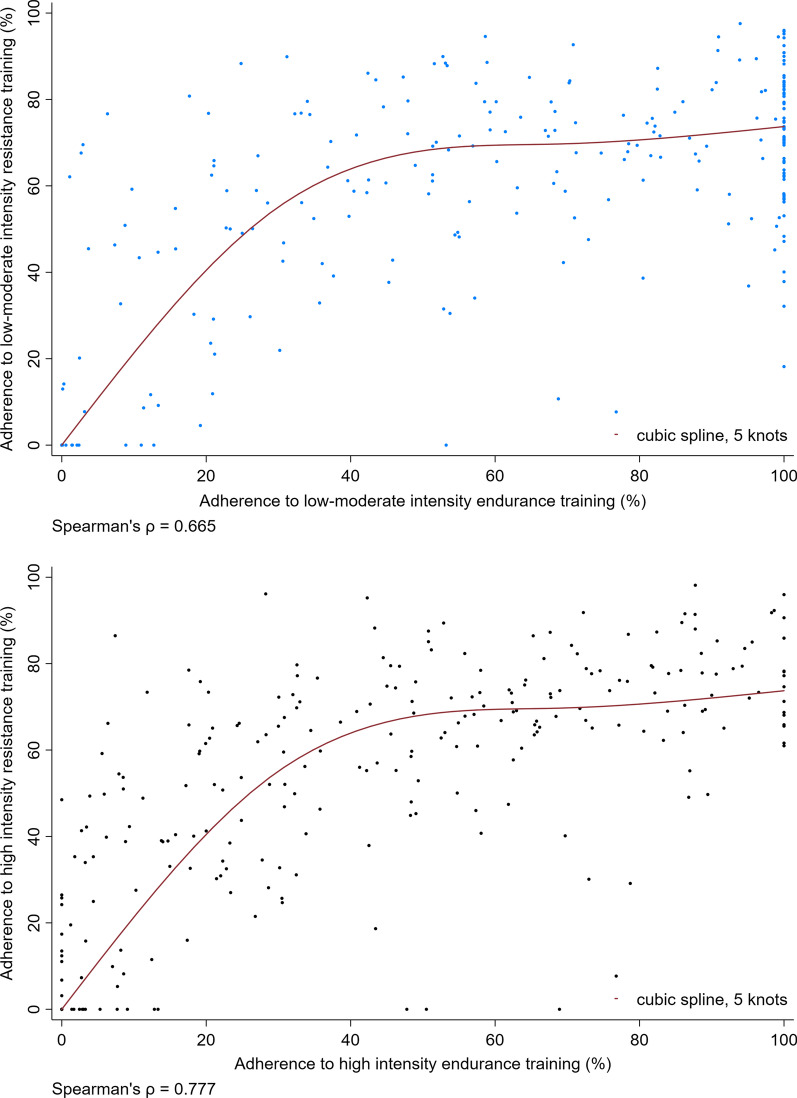
We found a positive curvilinear correlation between adherence to resistance and endurance training overall. A similar correlation was seen for adherence to frequency of resistance vs. endurance training in the HI group. In the HI group, adherence to resistance training intensity and time was > 80% for almost all participants. For endurance training adherence ranged from 0 to 100% for each of the FITT principles. Three clusters were identified, representing low, mixed, and high adherence to resistance and endurance training overall. Participants with higher age (Relative risk ratio [95% CI]; LMI: 0.86[0.77-0.96], HI: 0.83[0.74-0.93]), no behaviour change support (LMI: 0.11[0.02-0.56], HI: 0.20[0.05-0.85]), higher cardiorespiratory fitness (LMI: 0.81[0.69-0.94], HI: 0.80[0.69-0.92]), more fatigue (according to the reduced activity subscale of the MFI questionnaire) (LMI: 0.48[0.31-0.73], HI: 0.69[0.52-0.93]) or higher quality of life (LMI: 0.95[0.90-1.00], HI: 0.93[0.88-0.98]) were less likely to be in the low than the high adherence cluster whether randomised to LMI or HI training. Other determinants were specific to those randomised to LMI or HI training.
In an exercise intervention during cancer treatment, adherence to resistance and endurance training were positively correlated. Personalisation of interventions and additional support for some subgroups of participants may improve adherence. Trial registration NCT02473003 (clinicaltrials.gov, Registered 16/06/2015).
了解依从性对于提高癌症治疗期间运动干预的特异性至关重要。我们旨在同时确定对阻力训练和耐力训练干预的依从性;识别具有相似依从性特征的亚组;并研究这些亚组的决定因素。
在Phys-Can随机对照试验中,开始接受乳腺癌、结直肠癌或前列腺癌(新)辅助治疗的参与者(n = 577,81%为女性,平均(标准差)年龄59(12)岁,50%的人体质量指数(BMI)≥25kg/m²)被随机分配至为期6个月的高强度(HI)或低至中等强度(LMI)的、有监督的、基于小组的阻力训练以及个人在家进行的耐力训练,同时提供或不提供行为改变支持。依从性通过实际运动总量占规定运动总量的比例(0-100%)来计算,整体计算(HI组和LMI组)以及按照频率、强度、类型和时间(FITT原则)计算(HI组)。将阻力训练的依从性与耐力训练的整体依从性以及每项FITT原则的依从性进行绘图。采用K均值聚类分析来识别具有相似依从性特征的亚组。使用多项逻辑回归分析来研究亚组成员的潜在决定因素。
我们发现阻力训练和耐力训练的整体依从性之间存在正曲线相关性。在HI组中,阻力训练频率与耐力训练频率的依从性之间也存在类似的相关性。在HI组中,几乎所有参与者的阻力训练强度和时间的依从性均>80%。对于耐力训练,每项FITT原则的依从性范围为0至100%。识别出三个聚类,分别代表对阻力训练和耐力训练整体的低依从性、混合依从性和高依从性。年龄较大(相对风险比[95%置信区间];LMI组:0.86[0.77-0.96],HI组:0.83[0.74-0.93])、未获得行为改变支持(LMI组:0.11[0.02-0.56],HI组:0.20[0.05-0.85])、心肺适能较高(LMI组:0.81[0.69-0.94],HI组:0.80[0.69-0.92])、疲劳程度较高(根据MFI问卷的活动减少子量表)(LMI组:0.48[0.31-0.73],HI组:0.69[0.52-0.93])或生活质量较高(LMI组:0.95[0.90-1.00],HI组:0.93[0.88-0.98])的参与者,无论随机分配至LMI组还是HI组训练,与高依从性聚类相比,处于低依从性聚类的可能性较小。其他决定因素则特定于随机分配至LMI组或HI组训练的参与者。
在癌症治疗期间的运动干预中,阻力训练和耐力训练的依从性呈正相关。干预的个性化以及为部分参与者亚组提供额外支持可能会提高依从性。试验注册号NCT02473003(clinicaltrials.gov,2015年6月16日注册)。