Hanna Jonathan, Nargesi Arash A, Essien Utibe R, Sangha Veer, Lin Zhenqiu, Krumholz Harlan M, Khera Rohan
Department of Internal Medicine, Yale School of Medicine, New Haven, CT, USA.
Center for Health Equity Research and Promotion, VA Pittsburgh Healthcare System, Pittsburgh, PA, USA.
Am J Prev Cardiol. 2022 Aug 2;11:100370. doi: 10.1016/j.ajpc.2022.100370. eCollection 2022 Sep.
Cardioprotective antihyperglycemic agents, SGLT2 inhibitors (SGLT2i) and GLP-1 receptor agonists (GLP1RA), improve outcomes of patients with type 2 diabetes, but adoption has been limited. Differences across individuals have been noted but area-level variation is unknown.
Given healthcare access and sociodemographic differences, we evaluated whether SGLT2i and GLP-1RA utilization varies across US counties.
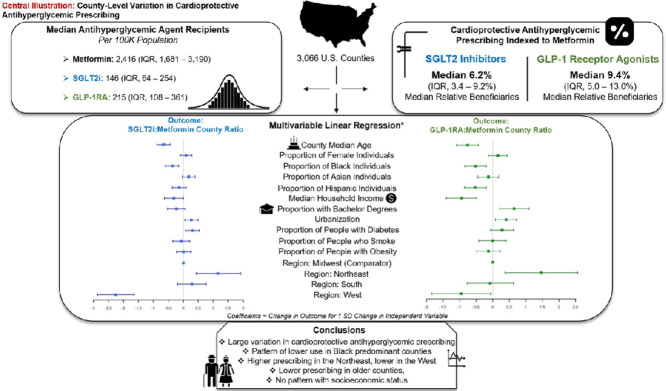
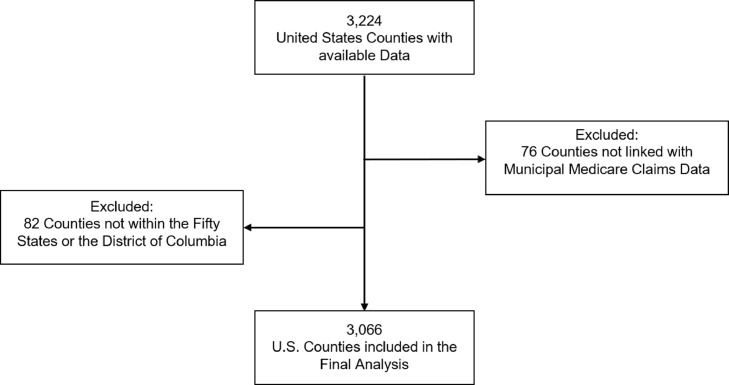
We linked 2019 Medicare Part D national prescription data with county-level demographic measures from the Agency for Health Quality and Research. We compared the number of beneficiaries receiving prescriptions for any cardioprotective antihyperglycemic to the number receiving metformin prescriptions across US counties. In multivariable linear regression with SGLT2i-to-metformin and GLP1RA-to-metformin prescriptions as outcomes, we evaluated county factors associated with use of cardioprotective agents while adjusting for sociodemographic measures, region, and cardiometabolic risk factor prevalence.
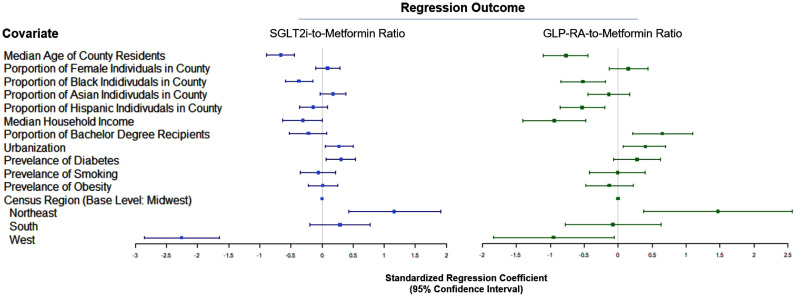
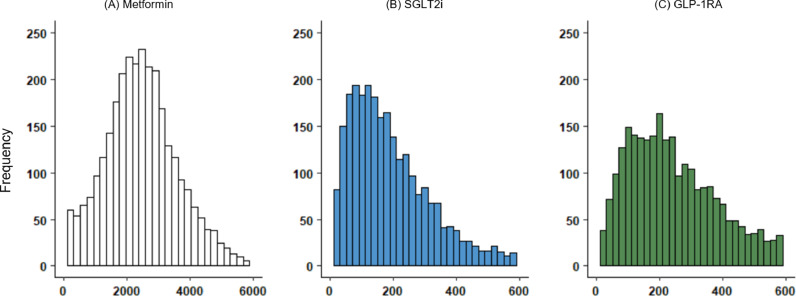
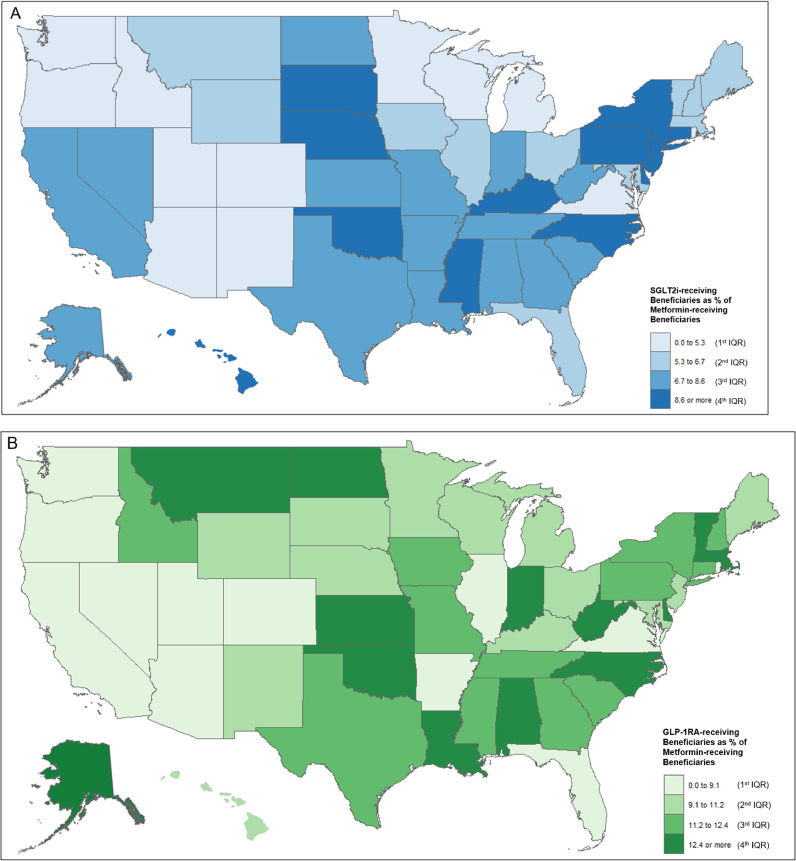
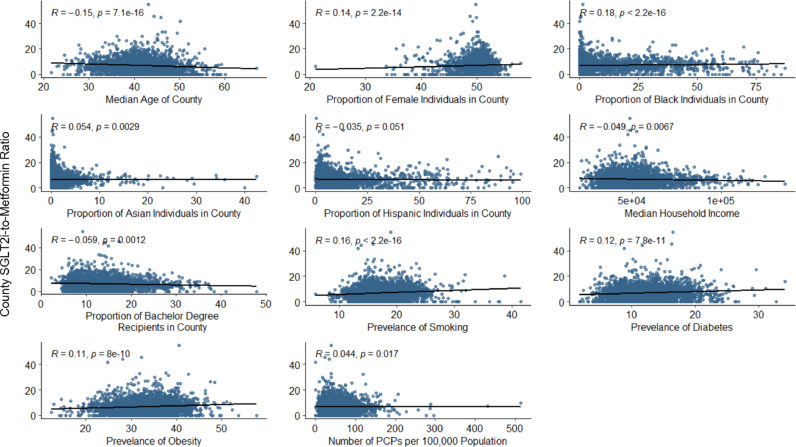
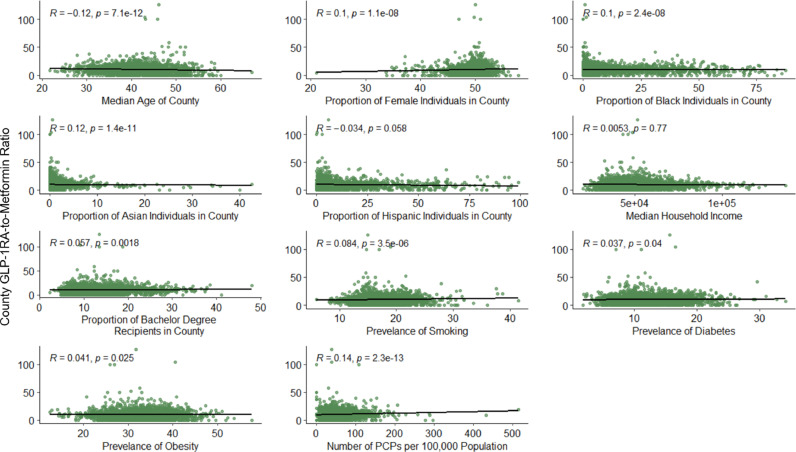
In 3066 US counties, there were a median 2,416 (IQR, 1681-3190) metformin-receiving beneficiaries per 100,000 population. A median 6.2% of beneficiaries receiving metformin received SGLT2i therapy, varying across counties (IQR, 3.4%-9.2%). A median 9.4% (IQR, 5.0%-13.0%) of beneficiaries receiving metformin received GLP-1RA. In adjusted analyses, higher percentage of Black population was associated with lower use at the county level of people on SGLT2i or GLP-1RA relative to metformin (a SD higher proportion of Black individuals with 0.4% [95% CI, -0.6% to -0.1%] and 0.5% [-0.8% to -0.2%] lower SGLT2i and GLP-1RA prescribing relative to metformin, respectively; < 0.01). A higher median age of county residents, rural location, and lower prevalence of diabetes were associated with lower SGLT2i prescribing. Similarly, more advanced age of county residents, rural location, proportion of Hispanic individuals, and household income and lower education levels were associated with lower GLP-1RA prescribing. Prescribing was higher in the Northeast and lower in the West as compared with the Midwest for both classes.
There was large variation by county in cardioprotective antihyperglycemic prescribing, with a pattern of lower use in Black-predominant and rural counties, highlighting the critical need to investigate equity in uptake of novel therapeutic agents.
具有心脏保护作用的降糖药物,即钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)和胰高血糖素样肽-1受体激动剂(GLP1RA),可改善2型糖尿病患者的预后,但应用有限。个体间的差异已被注意到,但地区层面的差异尚不清楚。
鉴于医疗保健可及性和社会人口统计学差异,我们评估了SGLT2i和GLP-1RA在美国各县的使用情况是否存在差异。
我们将2019年医疗保险D部分的全国处方数据与卫生质量与研究机构的县级人口统计学指标相联系。我们比较了美国各县接受任何具有心脏保护作用的降糖药物处方的受益人数与接受二甲双胍处方的人数。在以SGLT2i与二甲双胍以及GLP1RA与二甲双胍的处方数为结果的多变量线性回归分析中,我们评估了与心脏保护药物使用相关的县级因素,同时对社会人口统计学指标、地区和心血管代谢危险因素患病率进行了调整。
在美国的3066个县中,每10万人口中接受二甲双胍治疗的受益人的中位数为2416人(四分位间距,1681 - 3190人)。接受二甲双胍治疗的受益人中,接受SGLT2i治疗的比例中位数为6.2%,各县之间存在差异(四分位间距,3.4% - 9.2%)。接受二甲双胍治疗的受益人中,接受GLP-1RA治疗的比例中位数为9.4%(四分位间距,5.0% - 13.0%)。在调整分析中,黑人人口比例较高与县级SGLT2i或GLP-1RA相对于二甲双胍的使用比例较低相关(黑人个体比例标准差每增加1个单位,SGLT2i和GLP-1RA相对于二甲双胍的处方比例分别降低0.4%[95%置信区间,-0.6%至-0.1%]和0.5%[-0.8%至-0.2%];P < 0.01)。县居民年龄中位数较高、农村地区以及糖尿病患病率较低与SGLT2i处方量较低相关。同样,县居民年龄较大、农村地区、西班牙裔个体比例、家庭收入和教育水平较低与GLP-1RA处方量较低相关。与中西部地区相比,这两类药物在东北部的处方量较高,在西部较低。
各县在具有心脏保护作用的降糖药物处方方面存在很大差异,在黑人占主导的县和农村县使用量较低,这突出表明迫切需要调查新型治疗药物使用的公平性。