Department of Health Law, Policy, and Management, Boston University School of Public Health, Boston, Massachusetts.
Department of Health Policy, Vanderbilt University School of Medicine, Nashville, Tennessee.
JAMA Health Forum. 2021 Aug 27;2(8):e212291. doi: 10.1001/jamahealthforum.2021.2291. eCollection 2021 Aug.
Hepatitis C virus (HCV) can be cured with direct-acting antiviral medications, but state Medicaid programs often restrict access to these lifesaving medications owing to their high costs. Subscription-based payment models (SBPMs), wherein states contract with a single manufacturer to supply prescriptions at a reduced price, may offer a solution that increases access. Whether SBPMs are associated with changes in HCV medication use is unknown.
To estimate changes in Medicaid-covered HCV prescription fills after Louisiana and Washington implemented SBPMs on July 1, 2019.
This cross-sectional study examined trends in prescription fills of Medicaid-covered direct-acting antiviral HCV medications in Louisiana and Washington after implementation of SBPMs. A synthetic control approach was used to compare changes in HCV prescription fills between states that did and did not implement SBPMs. The unit of analysis was state-quarter. Outpatient direct-acting antiviral HCV prescription fills from the Medicaid State Drug Utilization Data files were obtained from all 50 US states and the District of Columbia from January 1, 2017, to June 30, 2020.
Implementation of SBPMs for Medicaid-covered direct-acting antiviral HCV medications.
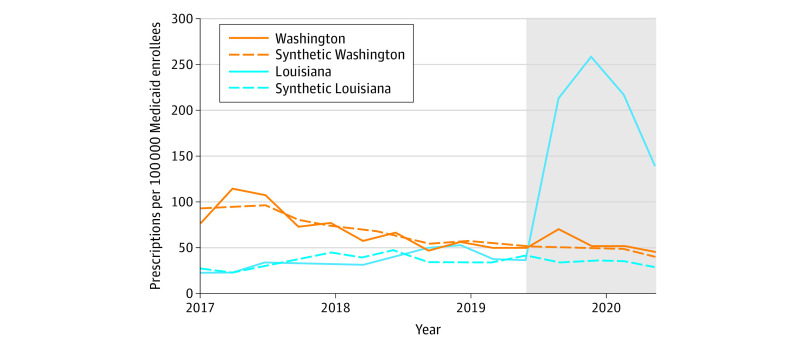
Direct-acting antiviral HCV prescriptions filled per 100 000 Medicaid enrollees.
In the year preceding SBPM implementation, the mean (SD) rate of quarterly HCV prescription fills per 100 000 Medicaid enrollees was 43.1 (8.6) prescriptions in Louisiana and 50.1 (4.1) in Washington. After SBPM implementation, the mean (SD) rate of quarterly HCV prescription fills per 100 000 enrollees was 206.0 (51.2) prescriptions in Louisiana and 53.9 (11.0) in Washington. In synthetic control models, SBPM implementation in Louisiana was associated with an increase of 173.5 (95% CI, 74.3-265.3) quarterly prescription fills per 100 000 Medicaid enrollees during the following year, a relative increase of 534.5% (95% CI, 228.7%-1125.0%). Washington did not experience a significant change in prescription fills following SBPM implementation.
In this cross-sectional study, Louisiana experienced substantial increases in HCV medication use among its Medicaid-enrolled population following SBPM implementation, whereas Washington did not. These differences may partially be explained by state-level variation in SBPM implementation, historical restrictions on access to HCV medications, and responses to the COVID-19 pandemic.
丙型肝炎病毒(HCV)可以用直接作用的抗病毒药物治愈,但由于其成本高,州医疗补助计划经常限制这些救命药物的获取。基于订阅的支付模式(SBPM),即各州与单一制造商签订合同,以降低价格供应处方,可能提供一种增加获取途径的解决方案。SBPM 是否与 HCV 药物使用的变化有关尚不清楚。
评估路易斯安那州和华盛顿州于 2019 年 7 月 1 日实施 SBPM 后,医疗补助覆盖的 HCV 处方填写情况的变化。
设计、地点和参与者:本横断面研究分析了路易斯安那州和华盛顿州实施 SBPM 后,医疗补助覆盖的直接作用抗病毒 HCV 药物的处方填写趋势。采用合成对照法比较了实施和未实施 SBPM 的州之间 HCV 处方填写的变化。分析单位为州季度。从 2017 年 1 月 1 日至 2020 年 6 月 30 日,从美国所有 50 个州和哥伦比亚特区的医疗补助州药物使用数据文件中获取直接作用抗病毒 HCV 药物的医疗补助覆盖的处方填写情况。
实施 SBPM 以覆盖 Medicaid 覆盖的直接作用抗病毒 HCV 药物。
每 10 万 Medicaid 参保人填写的直接作用抗病毒 HCV 处方数。
在实施 SBPM 之前的一年中,每 10 万 Medicaid 参保人每季度 HCV 处方填写的平均(SD)率为路易斯安那州 43.1(8.6)份,华盛顿州 50.1(4.1)份。实施 SBPM 后,每 10 万参保人每季度 HCV 处方填写的平均(SD)率为路易斯安那州 206.0(51.2)份,华盛顿州 53.9(11.0)份。在合成对照模型中,路易斯安那州实施 SBPM 后,在接下来的一年中,每 10 万 Medicaid 参保人每季度的处方填写量增加了 173.5(95%CI,74.3-265.3),相对增加了 534.5%(95%CI,228.7%-1125.0%)。华盛顿州在实施 SBPM 后,处方填写量没有明显变化。
在这项横断面研究中,路易斯安那州在实施 SBPM 后,其 Medicaid 参保人群的 HCV 药物使用量大幅增加,而华盛顿州则没有。这些差异可能部分归因于 SBPM 实施的州级差异、对 HCV 药物获取的历史限制以及对 COVID-19 大流行的反应。