Department of Health Law, Policy and Management, Boston University School of Public Health, Boston, Massachusetts.
Department of Health Policy, Vanderbilt University School of Medicine, Nashville, Tennessee.
JAMA Health Forum. 2021 Aug 27;2(8):e212285. doi: 10.1001/jamahealthforum.2021.2285. eCollection 2021 Aug.
Medicaid enrolls a disproportionate share of US adults with hepatitis C virus (HCV), and most receive Medicaid benefits through managed care organizations (MCOs). Medicaid MCOs often impose stricter requirements to access HCV medications than traditional fee-for-service Medicaid, which may inhibit use. Though Medicaid MCOs generally cover prescription drugs, several states have carved out direct-acting antiviral HCV medications from MCO coverage and opted to cover them under fee-for-service. Whether these carve outs were associated with changes in medication use is unknown.
To examine the association between Medicaid-covered HCV medication fills and carve outs of these medications from MCO coverage.
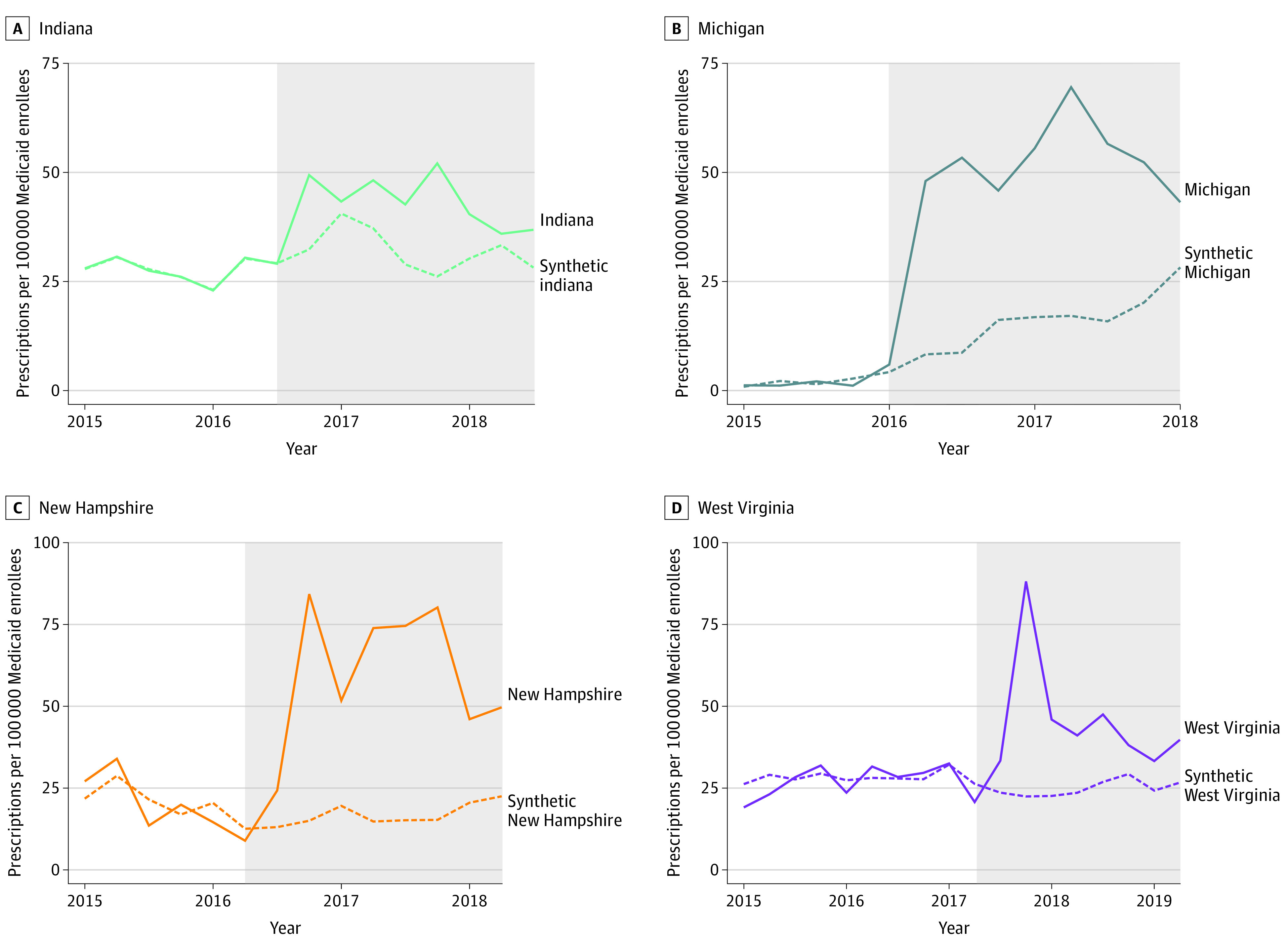
This cross-sectional study examined changes in fills of Medicaid-covered direct-acting antiviral HCV medications in 4 states (Indiana, Michigan, New Hampshire, and West Virginia) that carved out these drugs from Medicaid MCOs between 2015 and 2017. A synthetic control approach was used to compare changes in HCV prescription fills between states that did and did not carve out these medications from MCO prescription drug coverage. Data of direct-acting antiviral HCV prescription fills were obtained from the Medicaid State Drug Utilization Data files, January 2015 to June 2020. Data analysis was conducted from November 2020 to June 2021.
Carve outs of direct-acting antiviral HCV medications from Medicaid MCO prescription drug coverage.
Direct-acting antiviral HCV prescriptions filled per 100 000 Medicaid enrollees.
In this cross-sectional study, carve outs were associated with a mean quarterly increase of 22.1 (95% CI, 12.7-34.1) HCV prescriptions per 100 000 Medicaid enrollees, a relative increase of 86.3% compared with synthetic control states. Compared with each state's respective synthetic control, HCV prescription fills were associated with an increase of 11.5 (95% CI, 5.1-19.0) HCV prescription fills per 100 000 Medicaid enrollees per quarter in Indiana, 36.6 (95% CI, 23.5-53.9) in Michigan, 20.7 (95% CI, 11.1-32.8) in West Virginia, and 43.6 (95% CI, 25.9-68.4) in New Hampshire.
In this cross-sectional study of data from 39 states and the District of Columbia, carve outs of direct-acting antiviral HCV medications from Medicaid MCO prescription drug coverage were associated with significant increases in HCV medication use. Given their clinical benefits, greater uptake of HCV medication may help improve the health of Medicaid enrollees with HCV and reduce the economic burden of untreated HCV on the US health care system.
医疗补助计划(Medicaid)为美国成年丙型肝炎病毒(HCV)患者提供了不成比例的份额,其中大多数通过管理式医疗组织(MCO)获得医疗补助计划的福利。医疗补助计划 MCO 通常对获取 HCV 药物的要求比传统的按服务收费的医疗补助计划更为严格,这可能会抑制药物的使用。尽管医疗补助计划 MCO 通常涵盖处方药,但有几个州已经将直接作用抗病毒 HCV 药物从 MCO 覆盖范围中剔除,并选择按服务收费的方式进行覆盖。这些剔除是否与药物使用的变化有关尚不清楚。
研究医疗补助计划覆盖的 HCV 药物与这些药物从 MCO 覆盖范围中剔除之间的关联。
设计、设置和参与者:本横断面研究调查了 4 个州(印第安纳州、密歇根州、新罕布什尔州和西弗吉尼亚州)的 HCV 直接作用抗病毒药物的使用情况,这些州在 2015 年至 2017 年间将这些药物从 Medicaid MCO 处方药物覆盖范围中剔除。采用合成对照方法比较了这些州与未剔除这些药物的州之间 HCV 处方药物使用情况的变化。直接作用抗病毒 HCV 处方药物的使用数据来自于 Medicaid 州药物利用数据文件,时间范围为 2015 年 1 月至 2020 年 6 月。数据分析于 2020 年 11 月至 2021 年 6 月进行。
将直接作用抗病毒 HCV 药物从 Medicaid MCO 处方药物覆盖范围中剔除。
每 10 万医疗补助计划参保者中直接作用抗病毒 HCV 处方的数量。
在这项横断面研究中,剔除与每 10 万医疗补助计划参保者每季度 HCV 处方增加 22.1(95%CI,12.7-34.1)有关,与合成对照州相比,相对增加了 86.3%。与每个州各自的合成对照相比,印第安纳州每 10 万医疗补助计划参保者每季度 HCV 处方增加 11.5(95%CI,5.1-19.0),密歇根州增加 36.6(95%CI,23.5-53.9),西弗吉尼亚州增加 20.7(95%CI,11.1-32.8),新罕布什尔州增加 43.6(95%CI,25.9-68.4)。
在这项来自 39 个州和哥伦比亚特区的横断面研究中,将直接作用抗病毒 HCV 药物从 Medicaid MCO 处方药物覆盖范围中剔除与 HCV 药物使用的显著增加有关。鉴于它们的临床益处,更大程度地采用 HCV 药物可能有助于改善 HCV 参保者的健康状况,并减轻美国医疗保健系统中未治疗 HCV 的经济负担。