University of Minnesota Rural Health Research Center, Division of Health Policy and Management, University of Minnesota School of Public Health, Minneapolis.
Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor.
JAMA Health Forum. 2022 Mar 25;3(3):e220204. doi: 10.1001/jamahealthforum.2022.0204. eCollection 2022 Mar.
Rural obstetric unit closures are associated with adverse maternal and infant health outcomes and are most common among low-birth volume facilities located in remote areas. Declining access to obstetric care is a concern in rural communities in the US.
To assess rural hospital administrators' beliefs about safety, financial viability, and community need for offering obstetric care.
Using the American Hospital Association Annual Survey to identify rural hospitals with obstetric units, we developed and conducted a national survey of a sample of rural hospitals that provided obstetric services in 2021. Obstetric unit managers or administrators at 292 rural hospitals providing obstetric services were surveyed from March to August 2021.
Local factors, clinical safety, workforce, and financial considerations for obstetric services at participating hospitals.
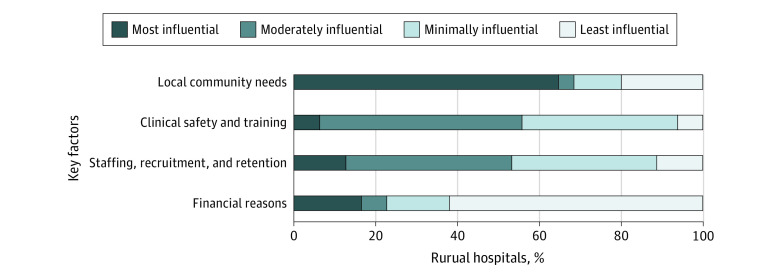
Hospital-level decisions on maintaining obstetric care.
Of the 93 total responding hospitals (32% response rate), 33 (35.5%) were critical access hospitals, 60 (64.5%) were located in micropolitan rural counties; they had a median (IQR) average daily census of 22 (10-53) patients, and 48 (52.2%) had experienced a recent decline in births, with a median (IQR) of 274 (120-446) births in 2019. Respondents reported that the minimum number of annual births needed to safely provide obstetric care was 200 (IQR, 100-350). From a financial perspective, the minimum number of annual births needed was also 200 (IQR, 120-360). When making decisions about maintaining obstetric care, 51 (64.6%) responding hospitals listed their highest priority as meeting local community needs, 13 (16.5%) listed financial considerations, and 10 (12.7%) listed staffing. Overall, 23 (25%) responding hospitals were not sure they would continue providing obstetrics, or they expected to stop offering this service.
In this survey of US rural hospitals that offer obstetric services, many administrators indicated prioritizing local community needs for obstetric care over concerns about financial viability and staffing.
农村产科单位的关闭与母婴健康不良结局有关,在位于偏远地区、低分娩量的设施中最为常见。在美国,农村社区获得产科护理的机会减少是一个令人关注的问题。
评估农村医院管理者对提供产科护理的安全性、财务可行性和社区需求的看法。
设计、地点和参与者:我们利用美国医院协会年度调查来确定具有产科单位的农村医院,并于 2021 年对提供产科服务的农村医院样本进行了全国性调查。2021 年 3 月至 8 月,对 292 家提供产科服务的农村医院的产科单位经理或管理人员进行了调查。
参与医院产科服务的当地因素、临床安全性、劳动力和财务考虑因素。
医院层面维持产科护理的决策。
在 93 家总回复医院中(32%的回复率),33 家(35.5%)为基层医疗保健医院,60 家(64.5%)位于农村小城市县;它们的平均(IQR)每日住院人数中位数(IQR)为 22(10-53)人,48 家(52.2%)最近经历了分娩量下降,2019 年的中位(IQR)分娩量为 274(120-446)人。受访者报告说,安全提供产科护理所需的最低年分娩量为 200(IQR,100-350)。从财务角度来看,所需的最低年分娩量也是 200(IQR,120-360)。在做出维持产科护理的决策时,51 家(64.6%)答复医院将满足当地社区需求列为首要任务,13 家(16.5%)将财务考虑因素列为首要任务,10 家(12.7%)将人员配备列为首要任务。总体而言,23 家(25%)答复医院不确定是否会继续提供产科服务,或者预计将停止提供这项服务。
在这项对提供产科服务的美国农村医院的调查中,许多管理人员表示,优先考虑当地社区对产科护理的需求,而不是对财务可行性和人员配备的担忧。